

AN EVALUATION THAT AIMS TO OPTIMIZE THE SHARED DECISION-MAKING PROCESS ABOUT DEFIBRILLATOR REPLACEMENT: A MULTI-METHOD APPROACH
Presented by Laurie Lamberton behalf of the Cardiovascular Evaluation UnitCADTH, 2018

2
Laurie J. Lambert, Lucy J. Boothroyd, Leila Azzi,
Caroline Collette, Philippe Brouillard,
Marie-Pascale Pomey, Monique Fournier,
Alexandre Grégoire, Isabelle Ganache, Anabèle Brière,
Peter Bogaty, Normand Racine, Michèle de Guise
THE INTER-DISCIPLINARY EVALUATION TEAM
3
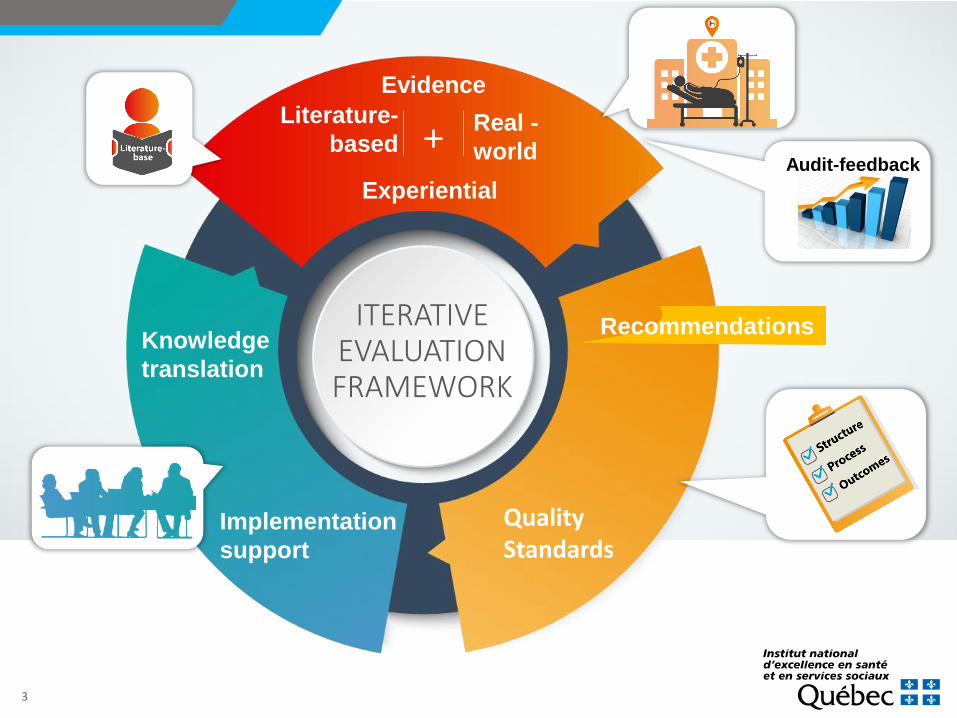
ITERATIVE EVALUATION FRAMEWORK
Literature-
basedReal -
world
Knowledge
translation
Recommendations
Implementation
support
Evidence
+Audit-feedback
Experiential
QualityStandards
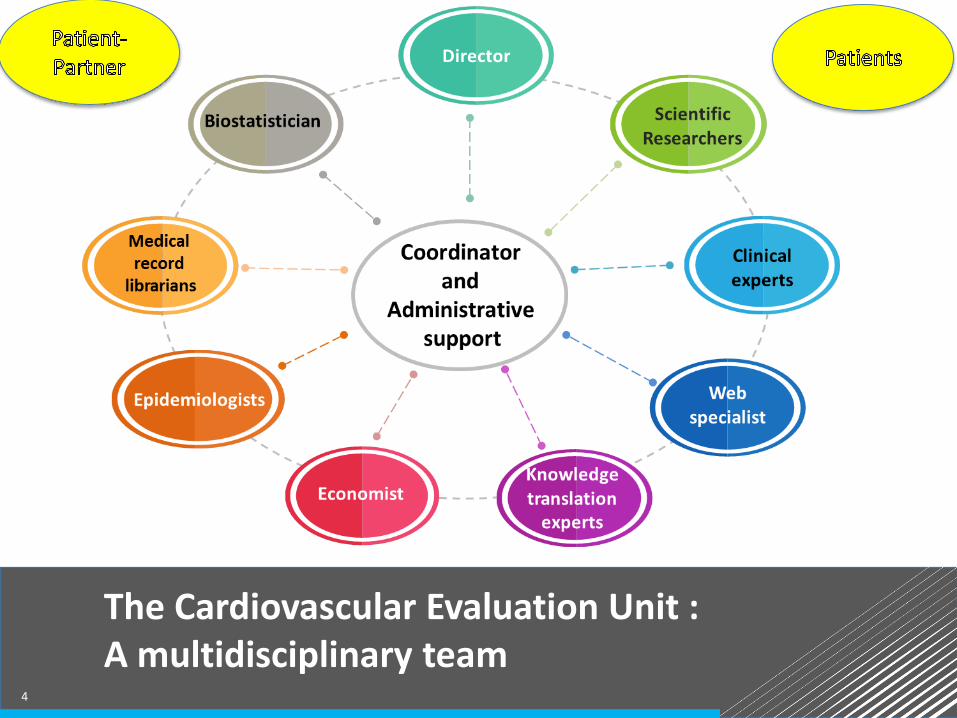
The Cardiovascular Evaluation Unit : A multidisciplinary team
4
5
BACKGROUND
• Malignant arrhythmias can occur unexpectedly and may result in sudden cardiac death
• An implantable cardioverter-defibrillator (ICD)
• produces an electrical therapy or shock when it detects a potentially malignant arrhythmia
• can produce inappropriate shocks
• is indicated in patients who have already had a malignant arrhythmia and survived or who are at risk of having a malignant arrhythmia
• requires generator replacement every 5 to 7 years to prevent complete depletion of the battery
• Should the ICD always be replaced ? How should we decide ?
6
Systematic review of the scientific literature concerningICD replacement:
• 2010-2017
• guidelines
• clinical studies
• qualitative studies of patient experience
• Two members of the scientific team independently selected publications and assessed study quality
•Data were extracted by one researcher and independently validated by a second
METHODS (1)
7
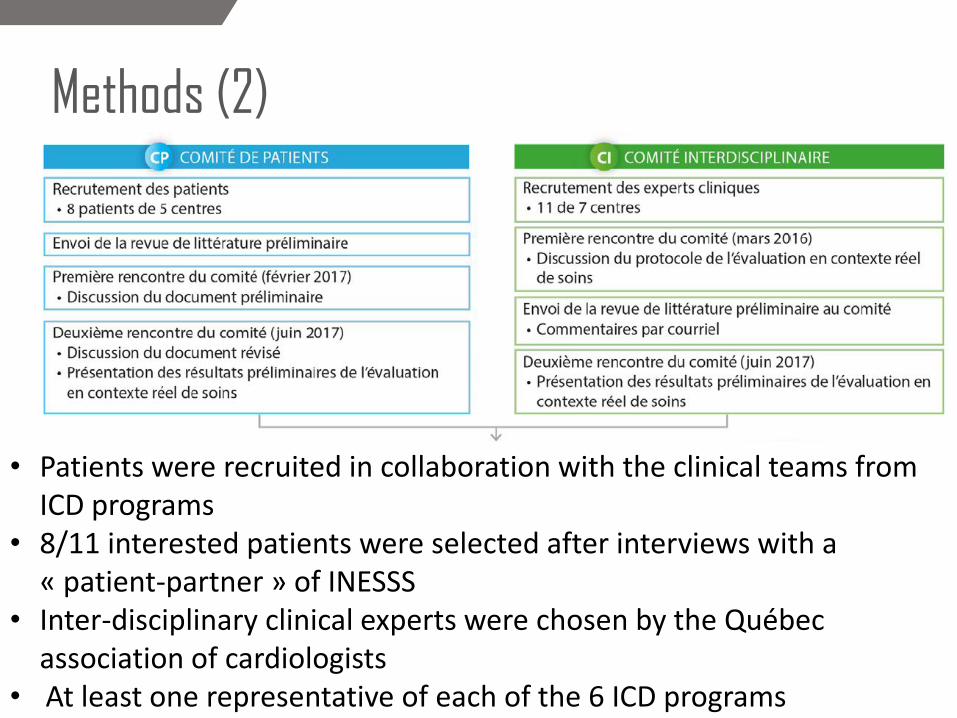
Methods (2)
• Patients were recruited in collaboration with the clinical teams fromICD programs
• 8/11 interested patients were selected after interviews with a « patient-partner » of INESSS
• Inter-disciplinary clinical experts were chosen by the Québec association of cardiologists
• At least one representative of each of the 6 ICD programs
8
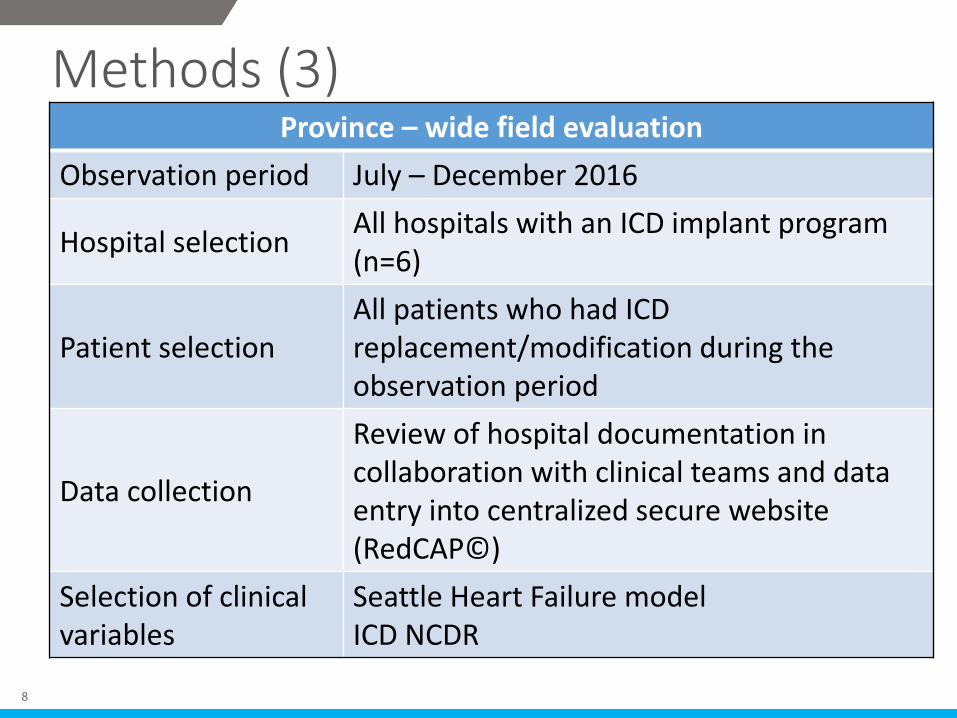
Methods (3)Province – wide field evaluation
Observation period July – December 2016
Hospital selectionAll hospitals with an ICD implant program (n=6)
Patient selectionAll patients who had ICD replacement/modification during the observation period
Data collection
Review of hospital documentation in collaboration with clinical teams and data entry into centralized secure website (RedCAP©)
Selection of clinical variables
Seattle Heart Failure model ICD NCDR
9
•No clinical guidelines for ICD replacement
•At first implant, an ICD is not clinically indicated for primary prevention patients with an ejection fraction (EF) >35 %
• improvement of EF is not uncommon, especially when patient eligible for CRT
• Incidence of appropriate ICD therapy is higher when EF is lower and patient has a history of appropriate therapy
KEY RESULTS FROM PUBLISHED LITERATURE

10
• In comparison with patients at time of ICD replacement, patients included in RCTs for primary prevention ICD were • younger • lower ejection fraction• fewer comorbidities• less than optimal medical therapy and no CRT
•With older age, the relative risk of dying from an arrhythmia, as opposed to some other cause, decreases
KEY RESULTS FROM PUBLISHED LITERATURE (2)
11
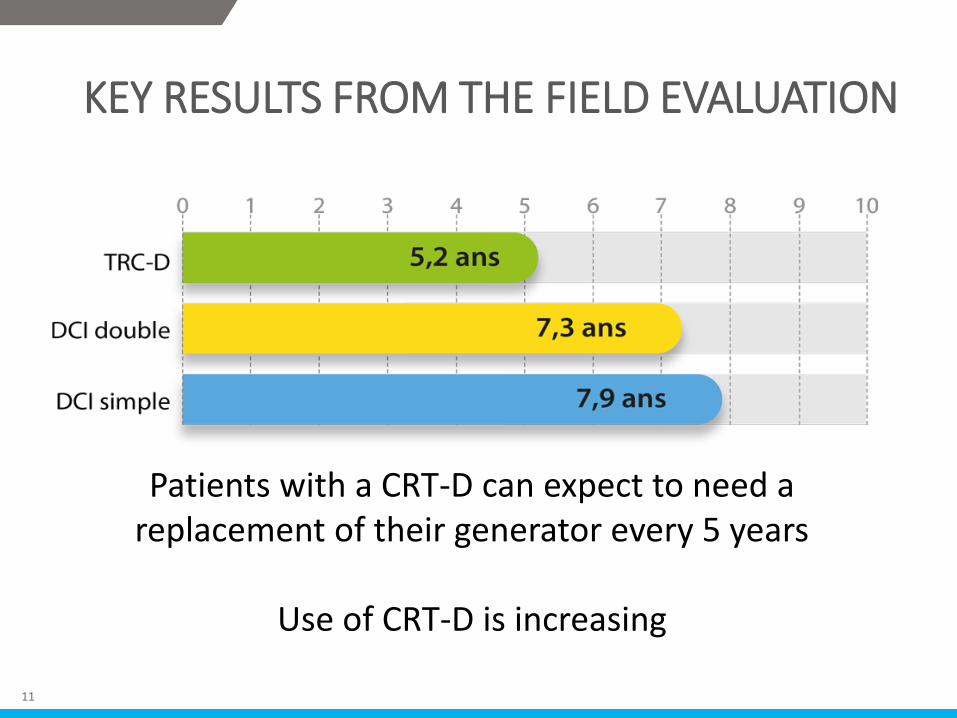
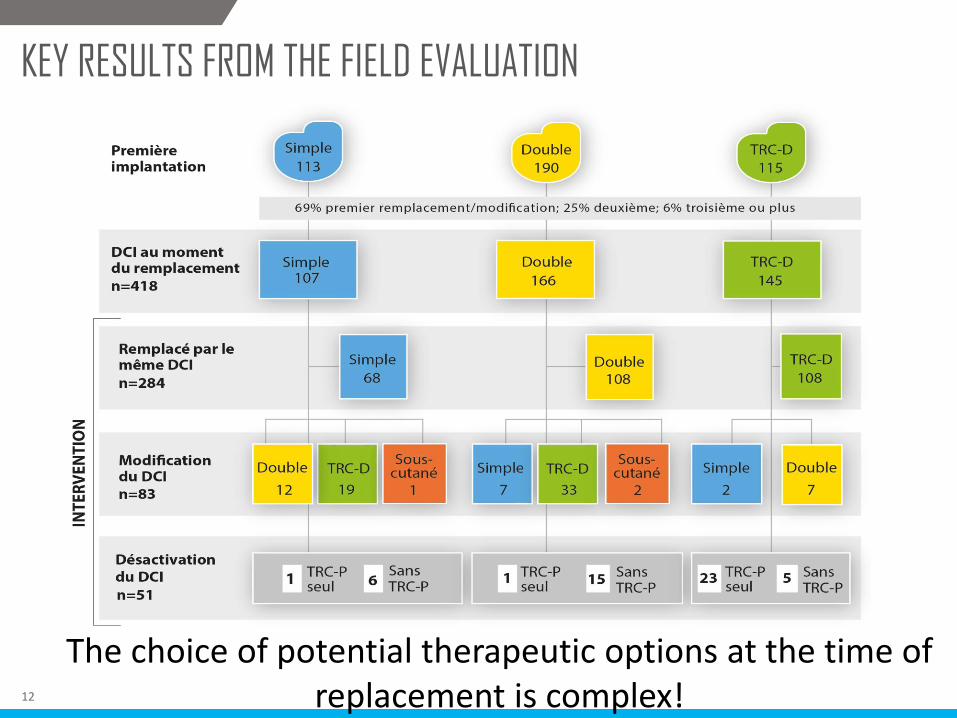
KEY RESULTS FROM THE FIELD EVALUATION
Patients with a CRT-D can expect to need a replacement of their generator every 5 years
Use of CRT-D is increasing
12
KEY RESULTS FROM THE FIELD EVALUATION
The choice of potential therapeutic options at the time of replacement is complex!
13
• 3 of 4 patients implanted for primary prevention had not received an appropriate therapy from their ICD at the time of decision for its replacement
• 32% of patients with CRT-D had an EF>35% at the time of ICD replacement
•Deactivation of the ICD function was not uncommon (12% of all interventions)
• 56% of patients who had a deactivation of their defibrillator function had an EF>35%
•Across Québec’s 6 ICD programs, the proportion of patients who had a deactivation of their defibrillator function varied from 3% to 20%
KEY RESULTS FROM THE FIELD EVALUATION

14
• Patient perception is that their ICD is saving their life and they have confidence in their doctor
• ICD implantation or modification has an important impact on loved ones
•Having time and a private space for sensitive deactivation discussions is important
• They received little information about their ICD and the need for replacements: expressed a need for better and more interactive ICD information tools
• They were unaware they had a “choice”
KEY RESULTS FROM PATIENT EXPERTS

15
•Main role of the electrophysiologist is to follow the device not the patient
• Electrophysiologist and treating doctor usually not the same person and often both have information relevant to the replacement decision
• patient’s treating doctor is often unknown
• lack of clinical information about the patient at the time of replacement and insufficient time to find out
• The decisions concerning ICD and CRT therapy are too complex to be explained in a decision tool
KEY RESULTS FROM CLINICAL EXPERTS

16
TRIANGULATION OF ALL THE INFORMATION
17
DEVELOPMENT OF RECOMMENDATIONS
• Two rounds of consultation by email with sharing of de-identifiedcomments amongst all members of the group
Êtes-vous d’accord? OUI ☐ ou NON ☐ Si NON, modifiez le texte en utilisant Suivi des modifications
Je m’abstiens de répondre ☐
Commentaires ou changements suggérés :
Patients Clinical experts
18
• Clinicians
• Patients
• INESSS evaluation team
• Presentation about shared decision-making for ICD replacement by a nurse-researcher fromOttawa (Krystina Lewis)
In-person meeting
DEVELOPMENT OF RECOMMENDATIONS
19
PRESENTLY UNDER MORATORIUM

20
• Diffusion of the reports:• Ministry• Satellite ICD clinics• All Québec heart failure clinics• 6 ICD implantation programs• Clinical associations (nurses, cardiologists etc)
• Presentations at clinical meetings:• Quebec Heart Failure Association • Canadian Cardiovascular Society
• Accredited workshops concerning shared decision-making and ICD replacement
• Creation of a support tool for ICD replacement and shareddecision-making
KNOWLEDGE TRANSLATION AND IMPLEMENTATIONSUPPORT
21
MEMORABLE QUOTES








