Thema: Biologika Teil 2: IL-17 und IL-23 Blockade Univ.-Prof. Dr. Matthias Augustin Direktor, Institut für Versorgungsforschung in der Dermatologie und bei Pflegeberufen und Hamburg Center for Health Economics Universitäres Psoriasis-Zentrum des UKE DDA-Zertifizierungsworkshop 06.09.2019
Transcript
Thema:
Biologika Teil 2: IL-17 und IL-23 Blockade
Univ.-Prof. Dr. Matthias AugustinDirektor, Institut für Versorgungsforschung in der
Dermatologie und bei Pflegeberufen und
Hamburg Center for Health Economics
Universitäres Psoriasis-Zentrum des UKE
DDA-Zertifizierungsworkshop 06.09.2019
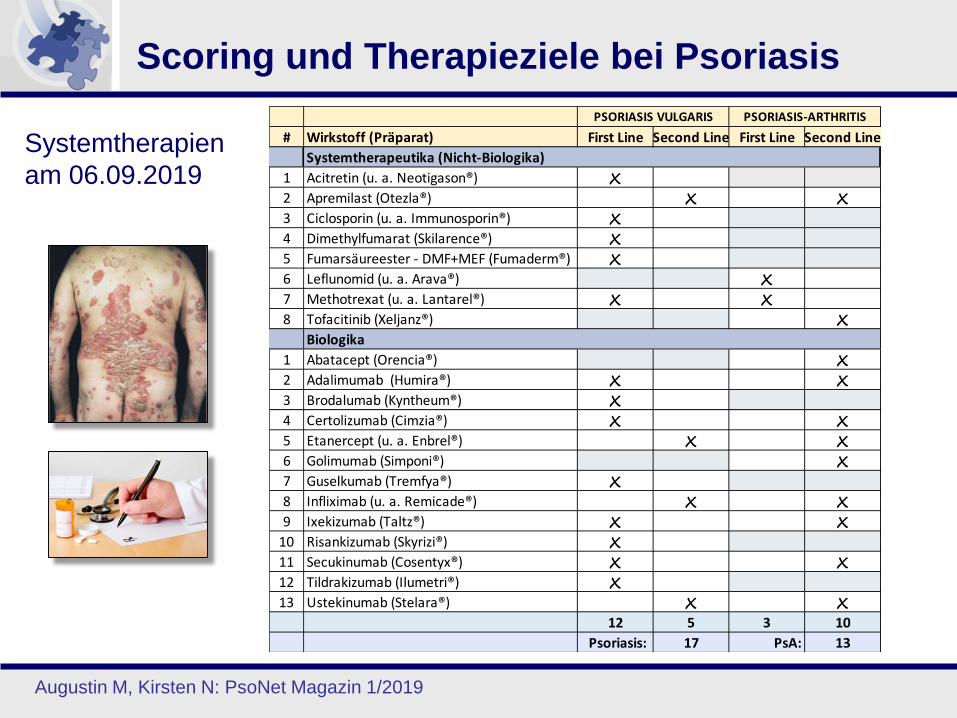
Scoring und Therapieziele bei Psoriasis
Systemtherapien
am 06.09.2019
Augustin M, Kirsten N: PsoNet Magazin 1/2019
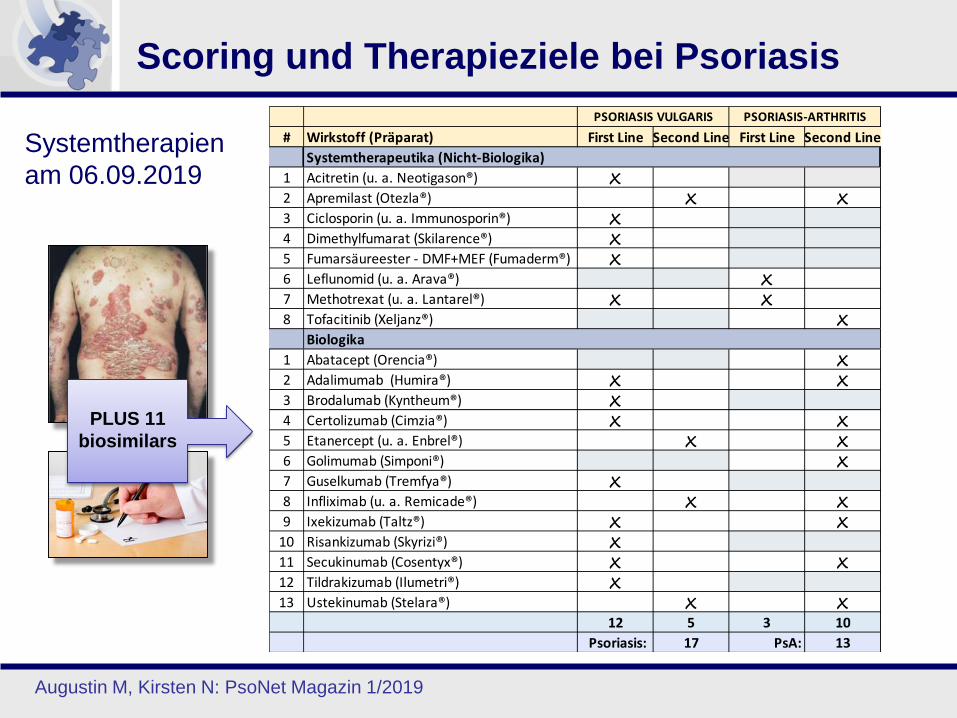
Scoring und Therapieziele bei Psoriasis
Systemtherapien
am 06.09.2019
Augustin M, Kirsten N: PsoNet Magazin 1/2019
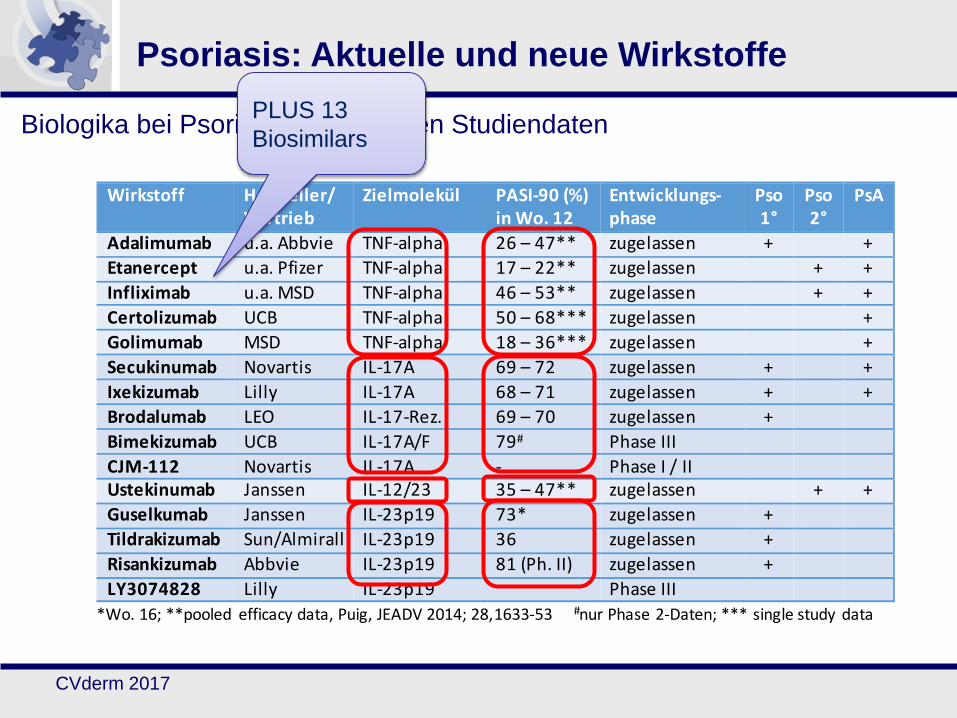
PLUS 11
biosimilars
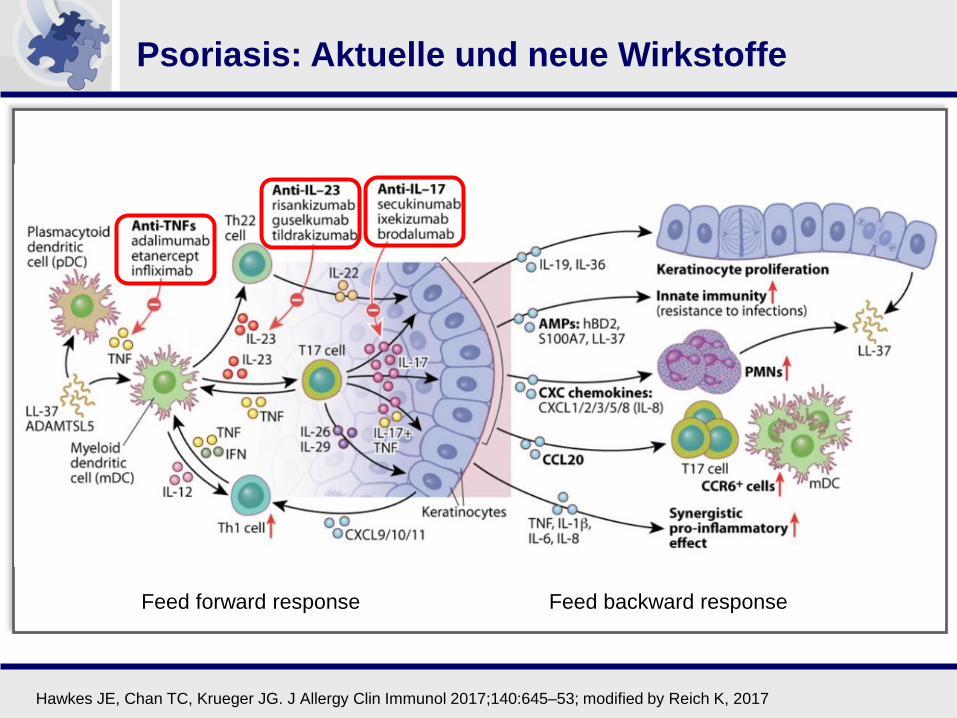
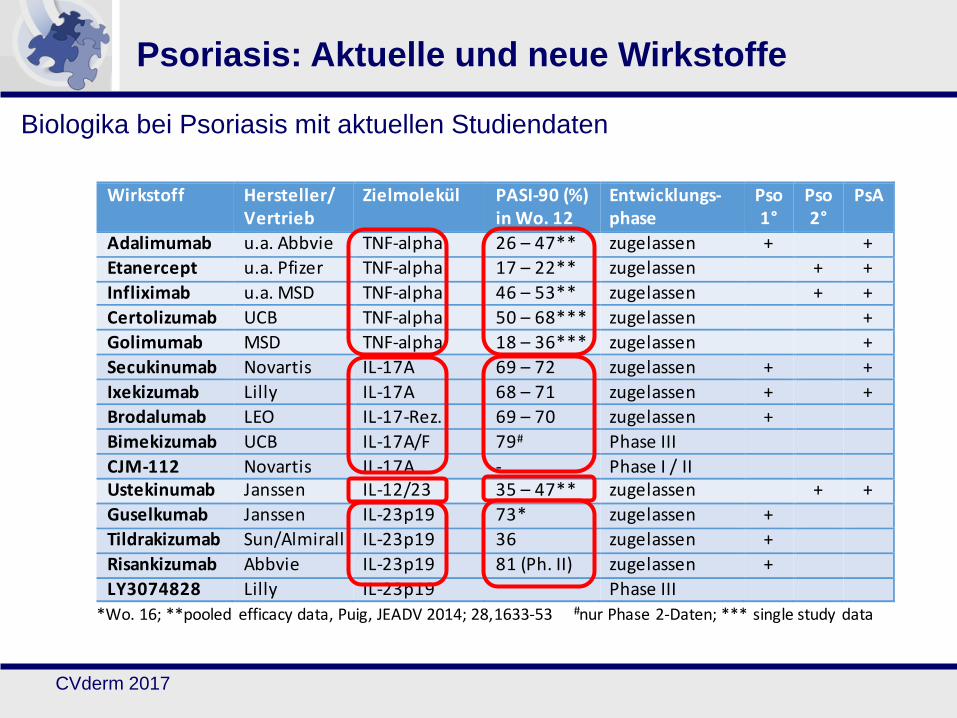
Psoriasis: Aktuelle und neue Wirkstoffe
Hawkes JE, Chan TC, Krueger JG. J Allergy Clin Immunol 2017;140:645–53; modified by Reich K, 2017
*P <0.0001 for comparisons of secukinumab vs. etanercept; †P <0.0001 for comparisons of secukinumab vs. placebo;‡P <0.001 for comparisons of secukinumab vs. etanercept; §P <0.001 for comparisons of secukinumab vs. placebo; primary endpoint at Week 12
No comparison with placebo was performed for PASI 100 because there were no patients with a response in the placebo group
Each piece of missing data is replaced with multiple values representing an overall distribution of the possible data (multiple imputation)
Adapted from Langley RG, et al. Poster presented at: International Congress of Psoriasis: From Gene to Clinic, London, UK, 2014. Poster #P99.
74.6%
70.6%
Res
po
nd
ers
(%
)
87.3%
72.8%
63.0%
66.2%
*†
*†
Week Week
49.3%
39.0%
34.0%
‡§
56.0%
‡§
PASI 90 ResponsePASI 75 Response PASI 100 Response
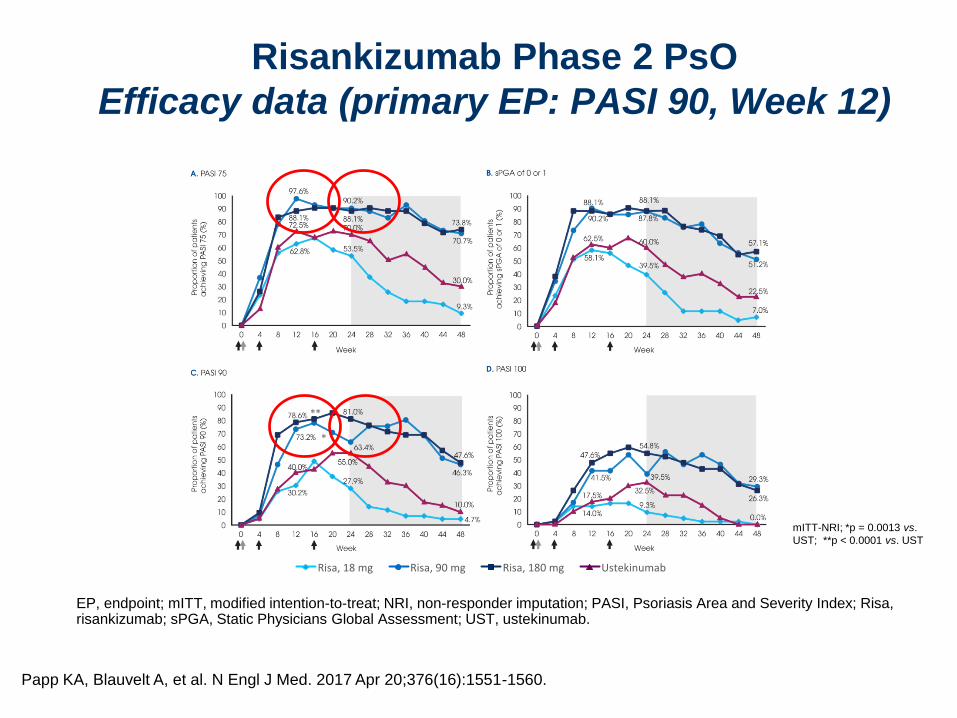
17
**
*
*
** * * *
* * * * * *
** p=0,0001, * p<0,0001 vs. Ustekinumab; multiple imputation
PA
SI 9
0-R
esp
on
der
(%)
Woche
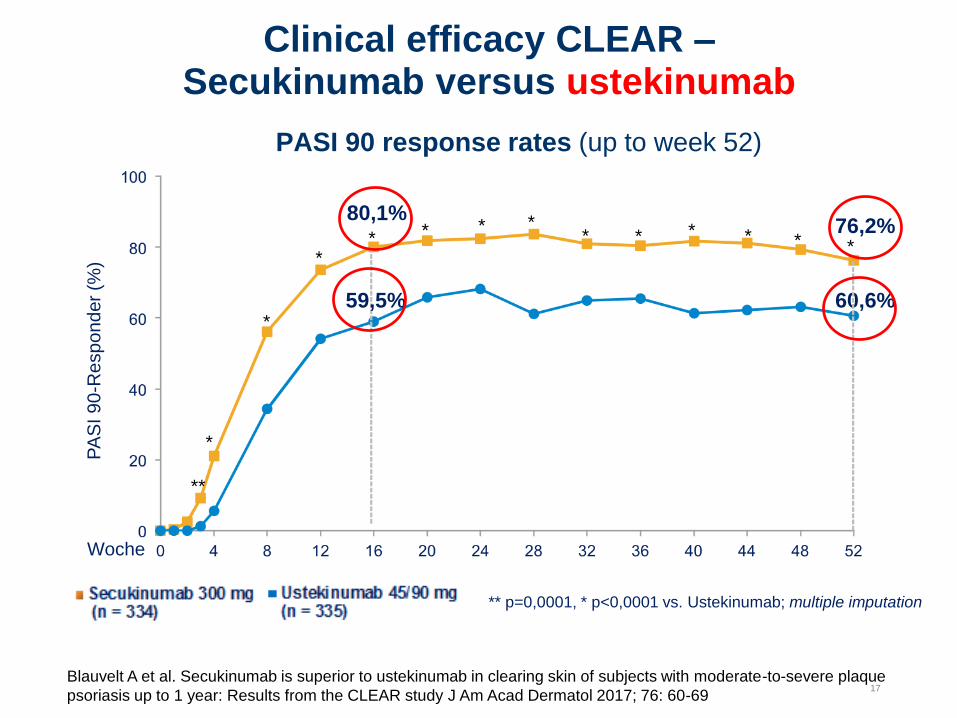
PASI 90 response rates (up to week 52)
----
----
----
----
----
----
----
----
----
----
----
-
76,2%
59,5%
80,1%
60,6%
----
----
----
----
----
----
----
----
----
----
----
17
Clinical efficacy CLEAR –Secukinumab versus ustekinumab
Blauvelt A et al. Secukinumab is superior to ustekinumab in clearing skin of subjects with moderate-to-severe plaque
psoriasis up to 1 year: Results from the CLEAR study J Am Acad Dermatol 2017; 76: 60-69
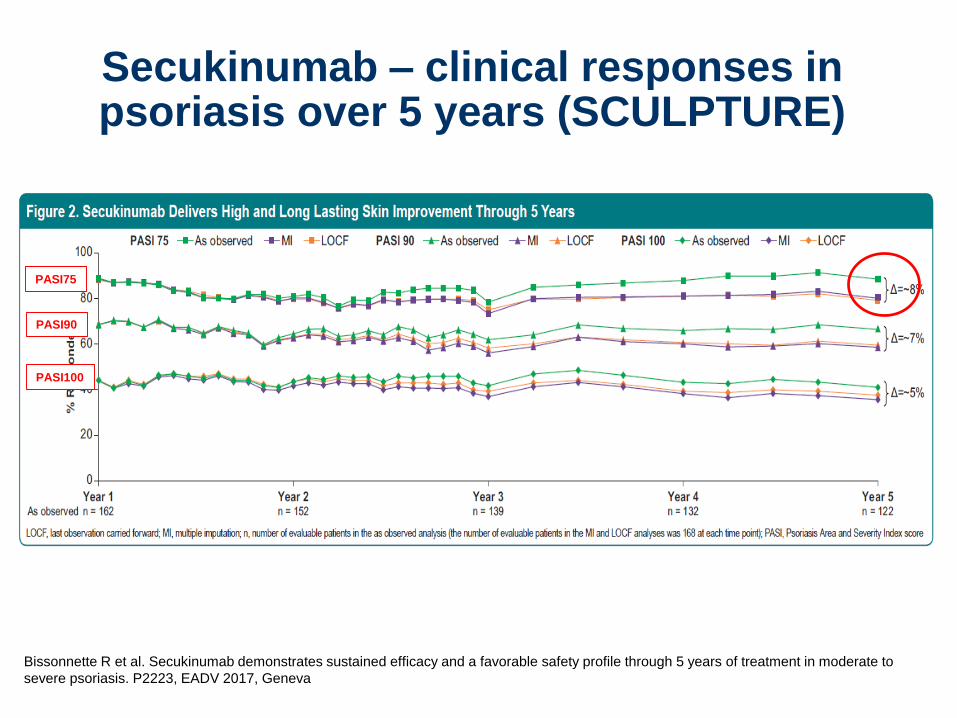
Secukinumab – clinical responses in psoriasis over 5 years (SCULPTURE)
Bissonnette R et al. Secukinumab demonstrates sustained efficacy and a favorable safety profile through 5 years of treatment in moderate to
severe psoriasis. P2223, EADV 2017, Geneva
PASI75
PASI90
PASI100
Secukinumab – clinical responses in psoriasis over 5 years (SCULPTURE)
Bissonnette R et al. Secukinumab demonstrates sustained efficacy and a favorable safety profile through 5 years of treatment in moderate to
severe psoriasis. P2223, EADV 2017, Geneva
P2223
Secukinumab Demonstrates High Sustained Efficacy and a Favorable Safety Profile Through
5 Years of Treatment in Moderate to Severe Psoriasis R Bissonnette,1 T Luger,2 D Thaçi,3 D Toth,4 A Lacombe,5 S Xia,6 R Mazur,5 M Patekar,5 P Charef,5 M Milutinovic,5 and C Leonardi7 1Innovaderm Research, Montreal, Canada;
2Department of Dermatology, University of Münster, Albert-Schweitzer-Campus, Münster, Germany;
3Comprehensive Center for Inflammation Medicine, University Hospital Schleswig-Holstein,
Lübeck, Germany; 4Probity Medical Research and XLR8 Medical Research, Windsor, Canada;
• Psoriasis is a chronic immune-mediated skin disease usually requiring
long term management
• Secukinumab, a fully human monoclonal antibody that neutralizes IL-17A,
has been shown to have significant efficacy in the treatment of moderate
to severe psoriasis and psoriatic arthritis, demonstrating sustained and
long lasting high levels of efficacy with a favorable safety profile1-5
• This secukinumab analysis is the first phase 3 study of an IL-17A inhibitor
evaluating efficacy and safety up to 5 years of treatment at the approved
dose
METHODS
• In the core SCULPTURE study, patients that were Psoriasis Area and
Severity Index (PASI) 75 responders at Week (Wk) 12 continued receiving
subcutaneous secukinumab 300 mg every 4 Wks until Year 1 (n=168 at
Wk 52) (Figure 1)
• Patients subsequently entered the extension phase (NCT01640951)
and continued the same double-blinded treatment regimen to Year 3,
and thereafter un-blinded to Year 5 (n=126 at Wk 260)
• No additional therapies (topicals) were permitted in the extension study
• Here we report final PASI 75/90/100 and absolute PASI ≤1/≤2/≤3
responses, dermatology life quality index (DLQI) 0/1 response (no impact
of skin disease on subject’s quality of life), and safety/tolerability through
5 years of treatment for the secukinumab 300 mg fixed interval arm only,
which is the recommended labelled dose regimen
• Efficacy data are reported as observed unless otherwise stated; multiple
imputation (MI) and last observation carried forward (LOCF) data are
reported for PASI responses as additional supportive analyses. Safety
events are analyzed per year using exposure adjusted incidence rates
(per 100 patient-years)
Double - blind Open-label
(Mostly home drug administration)
BL(Weeks) 52
Secukinumab 300 mg Fixed-interval
104 15612 208 260
N=168 N=155 N=141 N=134 N=126
Secukinumab
300 mg
Secukinumab 300 mg Retreatment-as-needed
Secukinumab 150 mg Fixed-interval Secukinumab
150 mg
Secukinumab 150 mg Retreatment-as-needed
Secukinumab 300 mg Retreatment-as- eeded
Secukinumab 150 mg Fixed-inter alSecukinumab
150 mg
Secukinumab 150 mg Retreatment-as- eeded
99.5% treatment compliance*
RESULTS
Baseline characteristics and subject disposition
• On completion of the 1-year core study, 168 subjects in the 300 mg cohort
entered the extension study
• Baseline demographics and clinical characteristics of extension study
subjects are presented in Table 1
• The mean PASI score of 23.5, percentage BSA involvement of 33.1% and
mean DLQI of 13.1, indicated a high disease severity at baseline
• At the end of Year 5, 126 subjects had completed the treatment phase of
the study and 42 had discontinued treatment (Table 2)
Efficacy
• PASI 75, 90 and 100 response rates sustained from Year 1 (88.9%, 68.5%
and 43.8%, respectively) to Year 5 (88.5%, 66.4% and 41%) (Figure 2)
– Similarly, PASI 75, 90 and 100 response rates sustained to Year 5
in the MI (80.1%, 58.6% and 35.6%) and LOCF (79.2%, 59.5% and
37.5%) analyses (Figure 2)
– PASI responses were consistent across the different analyses
undertaken (Figure 2)
• Secukinumab on average improved psoriasis by 90% through 5 years; the
mean improvement in mean absolute PASI from baseline to Year 1 was
91.1%, and from baseline to Year 5 was 90.1%
• Absolute PASI ≤1/≤2/≤3 responses sustained from Year 1 (58.6%, 67.9%
and 74.1%, respectively) to Year 5 (53.3%, 66.4% and 75.4%) (Figure 3)
– Similarly, PASI ≤1/≤2/≤3 responses sustained to Year 5 in the MI (47%,
58.4% and 66.9%) and LOCF (48.2%, 60.1%, 69%) analyses
Figure 3. Secukinumab Delivers Sustained Improvements in Psoriasis
Through 5 Years
0
20
% R
es
po
nd
ers
40
60
80
100
Year 1n = 162
Year 2n = 152
Year 3n = 139
Year 4n = 132
Year 5n = 122
PASI ≤3 PASI ≤2 PASI ≤1
74.1%
58.6%
67.9%75.4%
66.4%
53.3%
As observed analysis; n, number of evaluable patients; PASI, Psoriasis Area and Severity Index score
• Two thirds of patients reported no impact of skin disease on their lives
through 5 years of treatment; DLQI 0/1 responses were 72.7% at Year 1
and 65.5% at Year 5 (Figure 4)
0
20
DL
QI 0
/1 %
Res
po
nd
ers
40
60
80
100
Year 1n = 165
Year 2n = 153
Year 3n = 138
Year 4n = 132
Year 5n = 119
65.5%72.7%
Safety
• The safety profile of secukinumab remained favorable through 5 years of
treatment with no increase in yearly adverse event (AE) rates from Year 1
(Table 3)
• No new safety signals were identified and the safety profile was consistent
with that established in a large phase 3 program6
CONCLUSIONS
• Secukinumab treatment sustained high levels of skin clearance and
improvement in quality of life with a favorable safety profile through
5 years
– Average PASI improvement through 5 years was ~90%
– Patients experienced long lasting relief from the burden of psoriasis
– The safety profile was favorable with no increase of events over time
REFERENCES1. Hueber W et al. Sci Transl Med. 2010;2:52ra72.
2. Langley RG et al. N Engl J Med. 2014;371:326–338.
3. Thaci D et al. JAAD. 2015;73:400.
4. Blauvelt et al. JAAD. 2017;76:60–69.
5. Mease et al. N Engl J Med. 2015;373:1329–39.
6. van de Kerkhof et al. J Am Acad Dermatol. 2016;75(1):83–98.
ACKNOWLEDGMENTSAll authors participated in the development of the poster for presentation. The authors thank Brendan Marshall, PhD (Novartis Ireland Ltd.) for editorial and medical writing support, which was funded by Novartis Pharma AG, Switzerland in accordance with the Good Publication Practice (GPP3) guidelines (http://www.ismpp.org/gpp3).
ePoster presented: at 26th European Academy of Dermatology and Venereology Congress, September 13–17, 2017, Geneva, Switzerland
0
20
% R
es
po
nd
ers
40
60
80
100
Year 1n = 162As observed
Year 2n = 152
Year 3n = 139
Year 4n = 132
Year 5n = 122
As observedPASI 75 MI LOCF As observedPASI 90 MI LOCF As observedPASI 100 MI LOCF
Δ=~5%
Δ=~7%
Δ=~8%
Secukinumab – clinical responses in psoriasis over 5 years (SCULPTURE)
Bissonnette R et al. Secukinumab demonstrates sustained efficacy and a favorable safety profile through 5 years of treatment in moderate to
severe psoriasis. P2223, EADV 2017, Geneva
P2223
Secukinumab Demonstrates High Sustained Efficacy and a Favorable Safety Profile Through
5 Years of Treatment in Moderate to Severe Psoriasis R Bissonnette,1 T Luger,2 D Thaçi,3 D Toth,4 A Lacombe,5 S Xia,6 R Mazur,5 M Patekar,5 P Charef,5 M Milutinovic,5 and C Leonardi7 1Innovaderm Research, Montreal, Canada;
2Department of Dermatology, University of Münster, Albert-Schweitzer-Campus, Münster, Germany;
3Comprehensive Center for Inflammation Medicine, University Hospital Schleswig-Holstein,
Lübeck, Germany; 4Probity Medical Research and XLR8 Medical Research, Windsor, Canada;
• Psoriasis is a chronic immune-mediated skin disease usually requiring
long term management
• Secukinumab, a fully human monoclonal antibody that neutralizes IL-17A,
has been shown to have significant efficacy in the treatment of moderate
to severe psoriasis and psoriatic arthritis, demonstrating sustained and
long lasting high levels of efficacy with a favorable safety profile1-5
• This secukinumab analysis is the first phase 3 study of an IL-17A inhibitor
evaluating efficacy and safety up to 5 years of treatment at the approved
dose
METHODS
• In the core SCULPTURE study, patients that were Psoriasis Area and
Severity Index (PASI) 75 responders at Week (Wk) 12 continued receiving
subcutaneous secukinumab 300 mg every 4 Wks until Year 1 (n=168 at
Wk 52) (Figure 1)
• Patients subsequently entered the extension phase (NCT01640951)
and continued the same double-blinded treatment regimen to Year 3,
and thereafter un-blinded to Year 5 (n=126 at Wk 260)
• No additional therapies (topicals) were permitted in the extension study
• Here we report final PASI 75/90/100 and absolute PASI ≤1/≤2/≤3
responses, dermatology life quality index (DLQI) 0/1 response (no impact
of skin disease on subject’s quality of life), and safety/tolerability through
5 years of treatment for the secukinumab 300 mg fixed interval arm only,
which is the recommended labelled dose regimen
• Efficacy data are reported as observed unless otherwise stated; multiple
imputation (MI) and last observation carried forward (LOCF) data are
reported for PASI responses as additional supportive analyses. Safety
events are analyzed per year using exposure adjusted incidence rates
(per 100 patient-years)
Double - blind Open-label
(Mostly home drug administration)
BL(Weeks) 52
Secukinumab 300 mg Fixed-interval
104 15612 208 260
N=168 N=155 N=141 N=134 N=126
Secukinumab
300 mg
Secukinumab 300 mg Retreatment-as-needed
Secukinumab 150 mg Fixed-interval Secukinumab
150 mg
Secukinumab 150 mg Retreatment-as-needed
Secukinumab 300 mg Retreatment-as- eeded
Secukinumab 150 mg Fixed-inter alSecukinumab
150 mg
Secukinumab 150 mg Retreatment-as- eeded
99.5% treatment compliance*
RESULTS
Baseline characteristics and subject disposition
• On completion of the 1-year core study, 168 subjects in the 300 mg cohort
entered the extension study
• Baseline demographics and clinical characteristics of extension study
subjects are presented in Table 1
• The mean PASI score of 23.5, percentage BSA involvement of 33.1% and
mean DLQI of 13.1, indicated a high disease severity at baseline
• At the end of Year 5, 126 subjects had completed the treatment phase of
the study and 42 had discontinued treatment (Table 2)
Efficacy
• PASI 75, 90 and 100 response rates sustained from Year 1 (88.9%, 68.5%
and 43.8%, respectively) to Year 5 (88.5%, 66.4% and 41%) (Figure 2)
– Similarly, PASI 75, 90 and 100 response rates sustained to Year 5
in the MI (80.1%, 58.6% and 35.6%) and LOCF (79.2%, 59.5% and
37.5%) analyses (Figure 2)
– PASI responses were consistent across the different analyses
undertaken (Figure 2)
• Secukinumab on average improved psoriasis by 90% through 5 years; the
mean improvement in mean absolute PASI from baseline to Year 1 was
91.1%, and from baseline to Year 5 was 90.1%
• Absolute PASI ≤1/≤2/≤3 responses sustained from Year 1 (58.6%, 67.9%
and 74.1%, respectively) to Year 5 (53.3%, 66.4% and 75.4%) (Figure 3)
– Similarly, PASI ≤1/≤2/≤3 responses sustained to Year 5 in the MI (47%,
58.4% and 66.9%) and LOCF (48.2%, 60.1%, 69%) analyses
Figure 3. Secukinumab Delivers Sustained Improvements in Psoriasis
Through 5 Years
0
20
% R
es
po
nd
ers
40
60
80
100
Year 1n = 162
Year 2n = 152
Year 3n = 139
Year 4n = 132
Year 5n = 122
PASI ≤3 PASI ≤2 PASI ≤1
74.1%
58.6%
67.9%75.4%
66.4%
53.3%
As observed analysis; n, number of evaluable patients; PASI, Psoriasis Area and Severity Index score
• Two thirds of patients reported no impact of skin disease on their lives
through 5 years of treatment; DLQI 0/1 responses were 72.7% at Year 1
and 65.5% at Year 5 (Figure 4)
0
20
DL
QI 0
/1 %
Res
po
nd
ers
40
60
80
100
Year 1n = 165
Year 2n = 153
Year 3n = 138
Year 4n = 132
Year 5n = 119
65.5%72.7%
Safety
• The safety profile of secukinumab remained favorable through 5 years of
treatment with no increase in yearly adverse event (AE) rates from Year 1
(Table 3)
• No new safety signals were identified and the safety profile was consistent
with that established in a large phase 3 program6
CONCLUSIONS
• Secukinumab treatment sustained high levels of skin clearance and
improvement in quality of life with a favorable safety profile through
5 years
– Average PASI improvement through 5 years was ~90%
– Patients experienced long lasting relief from the burden of psoriasis
– The safety profile was favorable with no increase of events over time
REFERENCES1. Hueber W et al. Sci Transl Med. 2010;2:52ra72.
2. Langley RG et al. N Engl J Med. 2014;371:326–338.
3. Thaci D et al. JAAD. 2015;73:400.
4. Blauvelt et al. JAAD. 2017;76:60–69.
5. Mease et al. N Engl J Med. 2015;373:1329–39.
6. van de Kerkhof et al. J Am Acad Dermatol. 2016;75(1):83–98.
ACKNOWLEDGMENTSAll authors participated in the development of the poster for presentation. The authors thank Brendan Marshall, PhD (Novartis Ireland Ltd.) for editorial and medical writing support, which was funded by Novartis Pharma AG, Switzerland in accordance with the Good Publication Practice (GPP3) guidelines (http://www.ismpp.org/gpp3).
ePoster presented: at 26th European Academy of Dermatology and Venereology Congress, September 13–17, 2017, Geneva, Switzerland
0
20
% R
es
po
nd
ers
40
60
80
100
Year 1n = 162As observed
Year 2n = 152
Year 3n = 139
Year 4n = 132
Year 5n = 122
As observedPASI 75 MI LOCF As observedPASI 90 MI LOCF As observedPASI 100 MI LOCF
Δ=~5%
Δ=~7%
Δ=~8%
Fazit Secukinumab:
a) Gute Langzeitdaten
b) Vielseitige Wirksamkeit
c) Immunogenität kein Problem
d) Prediktorenstudie zu CV
outcomes
24
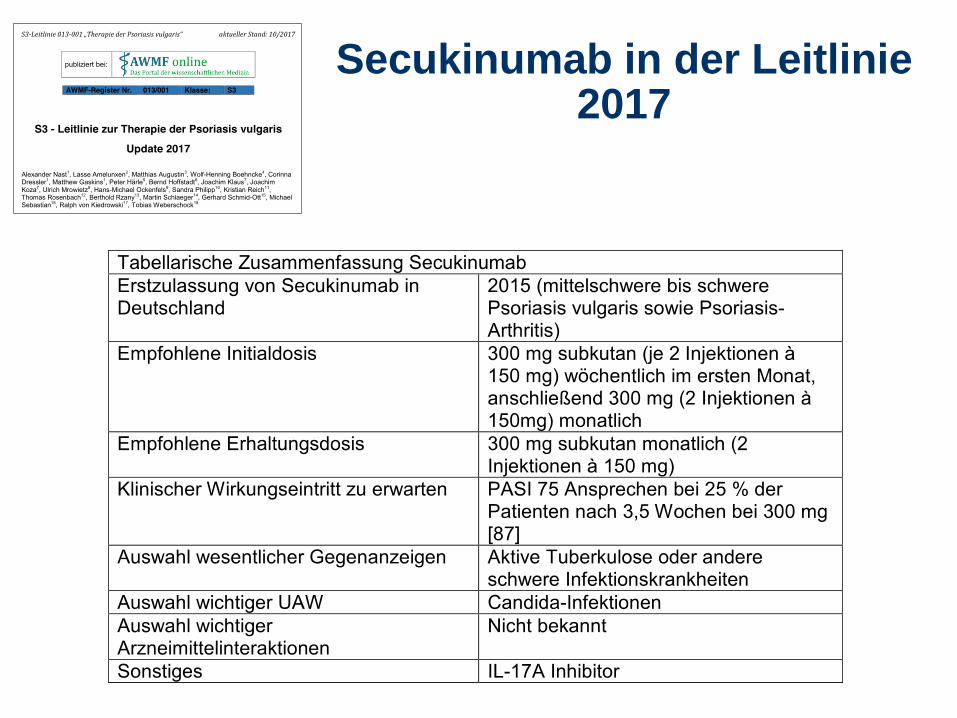
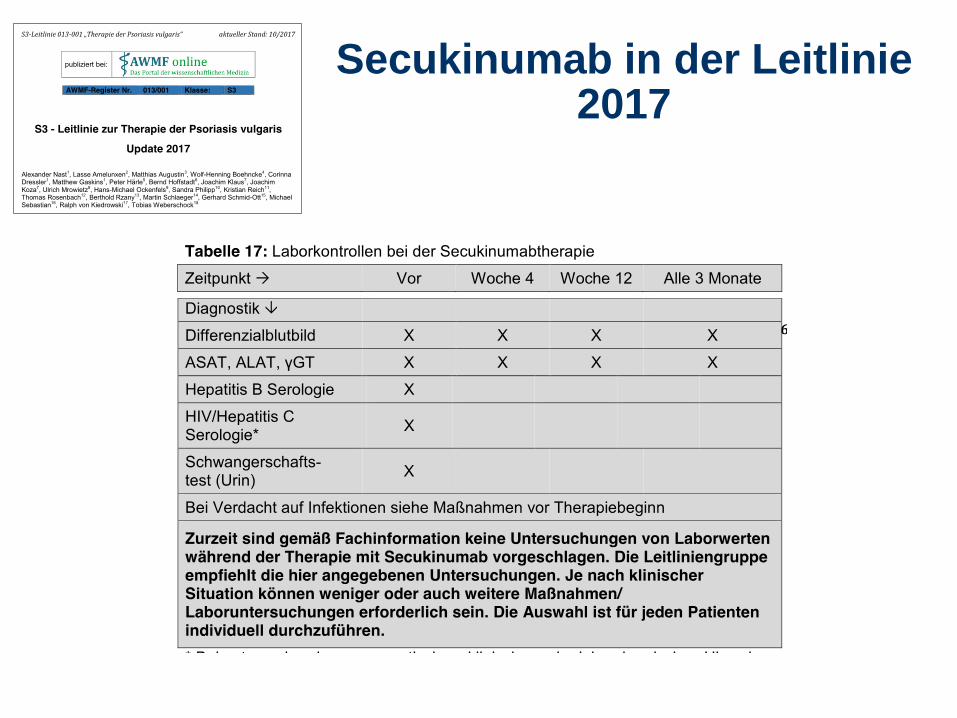
Secukinumab in der Leitlinie2017
25
Secukinumab in der Leitlinie2017
IL-17 inhibition Secukinumab
Ixekizumab
Brodalumab
Leitfragen:
Wie sehen die Langzeitdaten aus?
Welche Differenzierung zu Secukinumab?
Immunogenität?
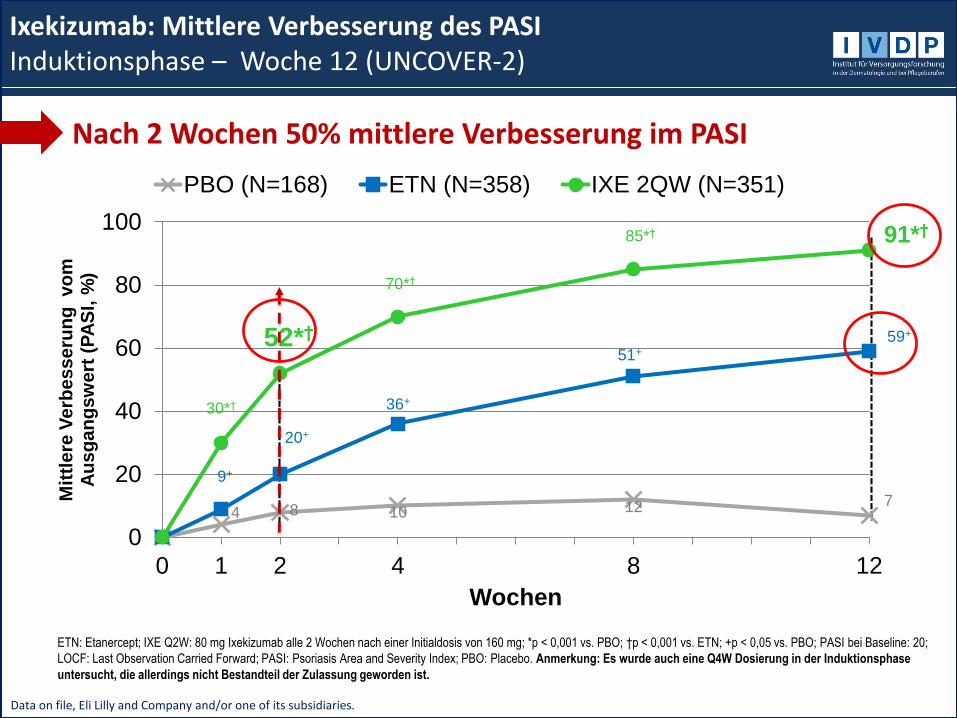
Ixekizumab bei Psoriasis
Data on file, Eli Lilly and Company and/or one of its subsidiaries.
ETN: Etanercept; IXE Q2W: 80 mg Ixekizumab alle 2 Wochen nach einer Initialdosis von 160 mg; *p < 0,001 vs. PBO; †p < 0,001 vs. ETN; +p < 0,05 vs. PBO; PASI bei Baseline: 20;
LOCF: Last Observation Carried Forward; PASI: Psoriasis Area and Severity Index; PBO: Placebo. Anmerkung: Es wurde auch eine Q4W Dosierung in der Induktionsphase
untersucht, die allerdings nicht Bestandteil der Zulassung geworden ist.
0
20
40
60
80
100
0 1 2 4 8 12
Mit
tle
re V
erb
es
se
run
g vo
m
Au
sg
an
gs
we
rt (
PA
SI,
%)
Wochen
PBO (N=168) ETN (N=358) IXE 2QW (N=351)
36+
51+
70*†
85*† 91*†
52*†
30*†
9+
20+
59+
4 8 10 12 7
Ixekizumab: Mittlere Verbesserung des PASI Induktionsphase – Woche 12 (UNCOVER-2)
Nach 2 Wochen 50% mittlere Verbesserung im PASI
In both studies, both IXE dose had higher PASI 90 by Week 2 compared to etanercept (p<0.001) and by Week 4 compared to placebo (p<0.001). In both
studies, both IXE dose groups had higher PASI 100 by Week 4 compared to etanercept (p<0.001) and placebo [p<0.01 (UNCOVER-2) and p<0.001
(UNCOVER-3)]; ITT-NRI
UNCOVER-2 and -3 Ixekizumab vs etanercept first 12 weeks
Griffiths C, Reich K, et al. Lancet 2015;386:541–51.
*p<.05, **p<.01, ***p<.001 by Fisher‘s exact test
IXE=Ixekizumab; NRI=Non-Responder Imputation; PASI=Psoriasis Area and Severity Index; UST=Ustekinumab
PASI 90 DLQI 0/1
IXORA-S Efficacy outcomes comparison ixekizumab vs. ustekinumab week 24, NRI
Reich et al. Br J Dermatol. 2017 May 19. doi: 10.1111/bjd.15666. [Epub ahead of print]; Supplement.
*P<0.05 vs IXE vs FAE; †P<0.05 IXE vs MTX; ‡P<0.05 MTX vs FAE
Nx, number of dropouts
Reich K, et al. EADV 2017; P1938
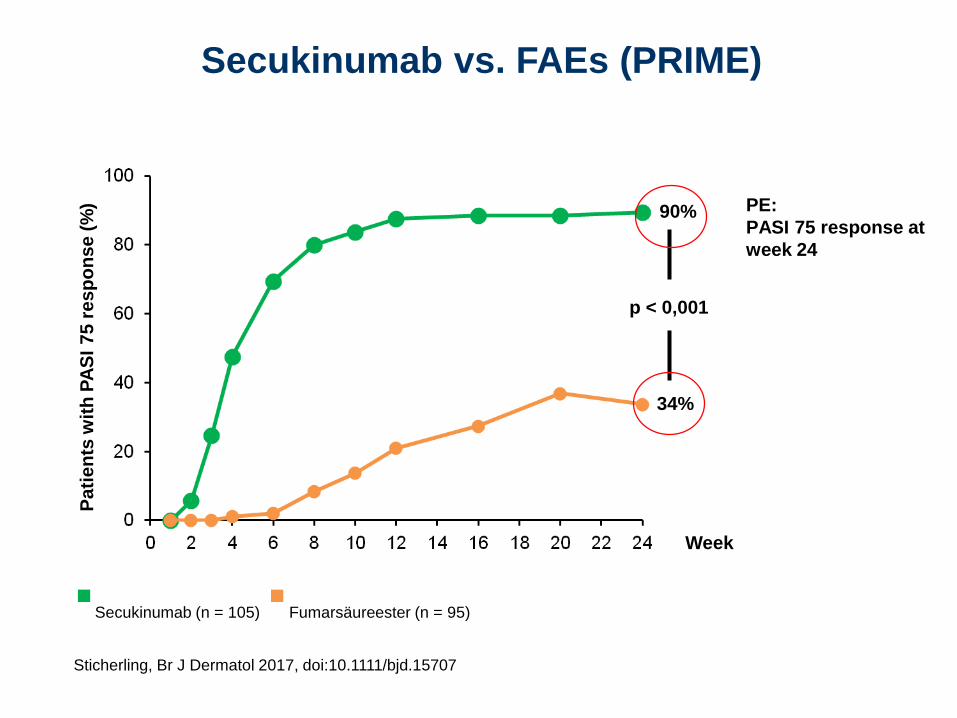
24-week, randomized open-label study: ixekizumab, fumaric acid esters, and methotrexate
in psoriasis patients naïve to systemic therapy
Primary endpoint: PASI 75 response over 24 weeks
FAE (n=54)
MTX (n=54)
IXE q2w/IXE q4w (n=54)
20
02
40
60
100
80
Pa
tie
nts
(%
)
4 6 8 10 12 140
Weeks
16 18 20 22 24
22.2
70.4
90.7*†‡
FAE (N=54, Nx=23)
MTX (N=54, Nx=49)
IXE q2w/IXE q4w (N=54, Nx=50)
20
02
40
60
100
80
Pa
tie
nts
(%
)
4 6 8 10 12 140
Weeks
16 18 20 22 24
52.2
77.6
98.0
NRI As observed
• Discontinued study before Week 24: FAE n=29; MTX n=3; IXE n=5
IXORA-S Ixekizumab vs. Ustekinumab
Results at EADV: nails and scalp
Comparison of ixekizumab and ustekinumab efficacy in
the treatment of nail lesions of patients with moderate
to severe plaque psoriasis: 24-week data of IXORA-S
trial1
Comparison of ixekizumab and ustekinumab in the treatment of
scalp psoriasis in patients with moderate-to-severe psoriasis:
24-week data from the IXORA-S trial2
1Dutronc et al. EADV 2017 OP03.01. 2Plummer et al. EADV 2017 P1928
Nagelpsoriasis (NAPSI) Kopfhautpsoriasis (PSSI)
IXORA-S Ixekizumab vs. Ustekinumab
Results at EADV: nails and scalp
Comparison of ixekizumab and ustekinumab efficacy in
the treatment of nail lesions of patients with moderate
to severe plaque psoriasis: 24-week data of IXORA-S
trial1
Comparison of ixekizumab and ustekinumab in the treatment of
scalp psoriasis in patients with moderate-to-severe psoriasis:
24-week data from the IXORA-S trial2
1Dutronc et al. EADV 2017 OP03.01. 2Plummer et al. EADV 2017 P1928
Nagelpsoriasis (NAPSI) Kopfhautpsoriasis (PSSI)
Fazit Ixekizumab:
a) Gute Langzeitdaten 2 J.
b) Breite klinische
Effektivität incl. Itch, Pain,
Nails, Scalp
• Taltz® is available as an autonjector or a prefilled syringe
• With each at a dosage of 80 mg Ixekizumab
• Easy for dosing:
Starting dose 2 Injections (2 x 80 mg)
1 Injection (80 mg) every 2 weeks during the induction phase (week 2-12)
1 Injection (80 mg) every 4 weeks during the maintenance period (starting at week 16)
Induction phase Maintenance
week
Dosierung Ixekizumab
IL-17 inhibition Secukinumab
Ixekizumab
Brodalumab
Leitfragen:
Wie sehen die Langzeitdaten aus?
Welche Differenzierung zu Secukinumab und
Ixekizumab?
Depression, Suizidalität?
PsA?
Brodalumab bei Psoriasis
*MACE: myocardial infarction (MI), stroke or CV death **ISR: injection site reactionsa 1 prostate cancer and 1 invasive papillary breast carcinoma
Russell CB, Rand H, Bigler J et al. Gene expression profiles normalized in psoriatic skin by treatment with brodalumab, a human anti-IL-17 receptor monoclonal antibody. J Immunol 2014;192:382836.Papp KA, Leonardi C, Menter A et al. Brodalumab, an antiinterleukin-17-receptor antibody for psoriasis. N Engl J Med 2012;366:1181-9.
PASI75 PASI100 85% 37%nach 12 Wochen
Brodalumab: Wirksamkeit nach 12 Wochen
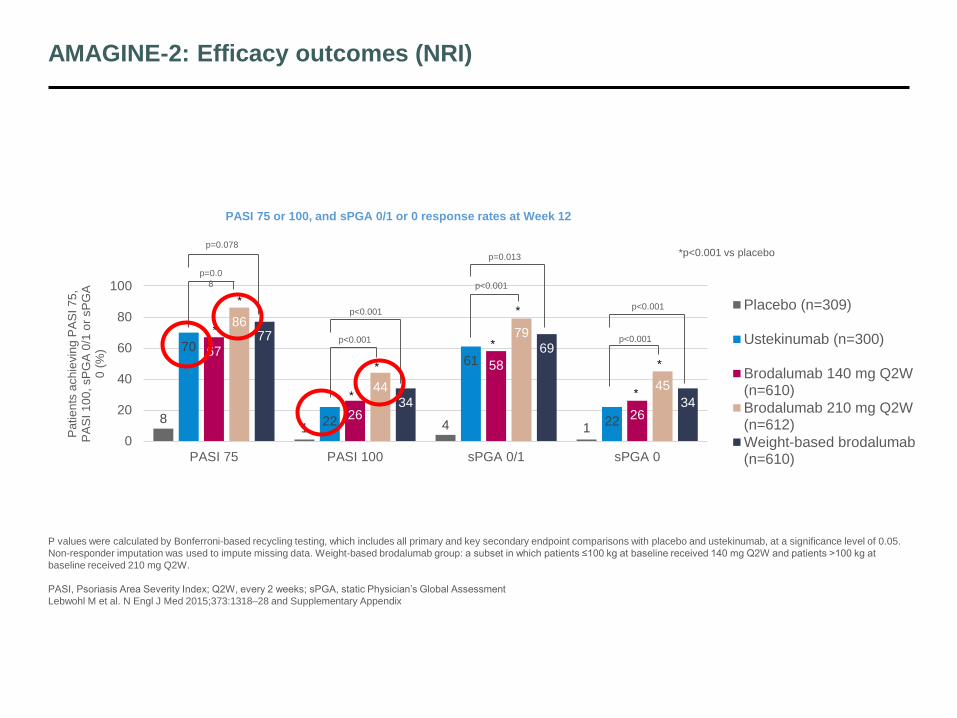
AMAGINE-2: Efficacy outcomes (NRI)
P values were calculated by Bonferroni-based recycling testing, which includes all primary and key secondary endpoint comparisons with placebo and ustekinumab, at a significance level of 0.05.
Non-responder imputation was used to impute missing data. Weight-based brodalumab group: a subset in which patients ≤100 kg at baseline received 140 mg Q2W and patients >100 kg at
baseline received 210 mg Q2W.
PASI, Psoriasis Area Severity Index; Q2W, every 2 weeks; sPGA, static Physician’s Global Assessment
Lebwohl M et al. N Engl J Med 2015;373:1318–28 and Supplementary Appendix
81 4 1
70
22
61
22
67
26
58
26
86
44
79
45
77
34
69
34
0
20
40
60
80
100
PASI 75 PASI 100 sPGA 0/1 sPGA 0
Pa
tie
nts
ach
ievin
g P
AS
I 7
5,
PA
SI
10
0, sP
GA
0/1
or
sP
GA
0
(%
)
Placebo (n=309)
Ustekinumab (n=300)
Brodalumab 140 mg Q2W(n=610)
Brodalumab 210 mg Q2W(n=612)
Weight-based brodalumab(n=610)
*
*
*
*
*
*
*
*
p=0.0
8
p<0.001
p<0.001
p<0.001
p<0.001
p=0.013
p<0.001
p=0.078
PASI 75 or 100, and sPGA 0/1 or 0 response rates at Week 12
*p<0.001 vs placebo
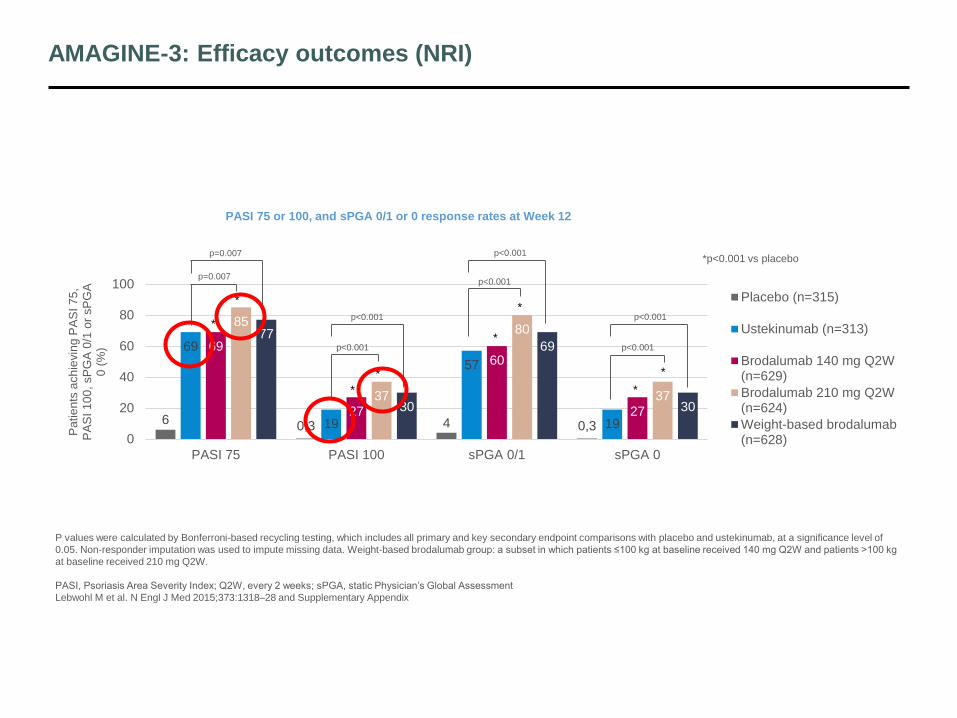
AMAGINE-3: Efficacy outcomes (NRI)
P values were calculated by Bonferroni-based recycling testing, which includes all primary and key secondary endpoint comparisons with placebo and ustekinumab, at a significance level of
0.05. Non-responder imputation was used to impute missing data. Weight-based brodalumab group: a subset in which patients ≤100 kg at baseline received 140 mg Q2W and patients >100 kg
at baseline received 210 mg Q2W.
PASI, Psoriasis Area Severity Index; Q2W, every 2 weeks; sPGA, static Physician’s Global Assessment
Lebwohl M et al. N Engl J Med 2015;373:1318–28 and Supplementary Appendix
60,3 4 0,3
69
19
57
19
69
27
60
27
85
37
80
37
77
30
69
30
0
20
40
60
80
100
PASI 75 PASI 100 sPGA 0/1 sPGA 0
Pa
tie
nts
ach
ievin
g P
AS
I 7
5,
PA
SI
10
0, sP
GA
0/1
or
sP
GA
0 (
%)
Placebo (n=315)
Ustekinumab (n=313)
Brodalumab 140 mg Q2W(n=629)
Brodalumab 210 mg Q2W(n=624)
Weight-based brodalumab(n=628)
*
*
*
*
*
*
*
*
p=0.007
p<0.001
p<0.001
p<0.001
p=0.007
p<0.001
p<0.001
p<0.001
*p<0.001 vs placebo
PASI 75 or 100, and sPGA 0/1 or 0 response rates at Week 12
AMAGINE-1, -2 and -3: Efficacy of brodalumab in nail and scalp psoriasis
NAPSI score at Week 121
(multiple imputation)
Brodalumab
Placebo
n=261
140 mg
Q2W
n=466
210 mg
Q2W
n=472
NAPSI, mean (SE) 8.5 (0.3) 6.0 (0.2) 5.2 (0.2)
Tx difference vs placebo, least
squares mean (95% CI)-
2.5
(2.0–3.0)
3.3
(2.8–3.8)
p value vs placebo <0.001 <0.001
Nail psoriasis data are a pooled analysis of AMAGINE-1, -2 and -3.1 Scalp psoriasis data is analysis of AMAGINE-1; non-responder imputation was used to impute missing data.2 PSSI only summarised in subjects with baseline PSSI ≥15 and
SSA ≥30%.2 *p<0.001, †p=0.007 for comparisons between brodalumab and placebo groups.2
NAPSI, Nail Psoriasis Severity Index; PSSI, Psoriasis Scalp Severity Index; Q2W, every 2 weeks; SE, standard error1Lebwohl MG et al. P5296 Presented at 75th Annual Meeting of the American Academy of Dermatology, March 3-7, 2017, Orlando, FL;
2Yamauchi P et al. P5247 Presented at 75th Annual Meeting of the American Academy of Dermatology, March 3–7, 2017, Orlando, FL
11,6
37,546,3
0
10
20
30
40
50
Placebon=261
Brodalumab140 mg Q2W…
Brodalumab210 mg Q2W…
NA
PS
I sco
re
imp
rove
me
nt fr
om
b
ase
line
(%
)
Improvement in NAPSI score at Week 121
AMAGINE-1, -2 and -3 (as observed)
0
10
20
30
40
50
60
70
-3 2 7 12Pa
tie
nts
ach
ievin
g P
SS
I 1
00
(%
)
WeekPlacebo
63.4%
41.0%
3.2%
*
*
*
*
**
*
†
PSSI 100 response rates through Week 122
AMAGINE-1 (NRI)
1) Nails 2) Scalp
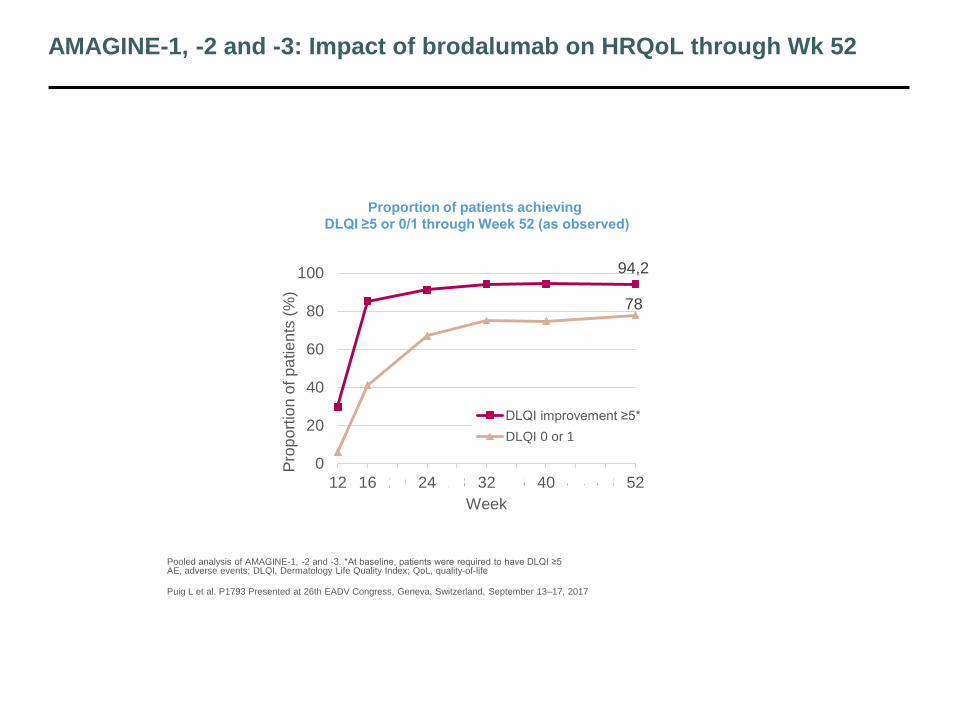
AMAGINE-1, -2 and -3: Impact of brodalumab on HRQoL through Wk 52
Pooled analysis of AMAGINE-1, -2 and -3. *At baseline, patients were required to have DLQI ≥5AE, adverse events; DLQI, Dermatology Life Quality Index; QoL, quality-of-life
Puig L et al. P1793 Presented at 26th EADV Congress, Geneva, Switzerland, September 13–17, 2017
94,2
78
0
20
40
60
80
100
12 16 20 24 28 32 36 40 44 48 52
Pro
po
rtio
n o
f p
atie
nts
(%
)
Week
DLQI improvement ≥5*
DLQI 0 or 1
Proportion of patients achieving
DLQI ≥5 or 0/1 through Week 52 (as observed)
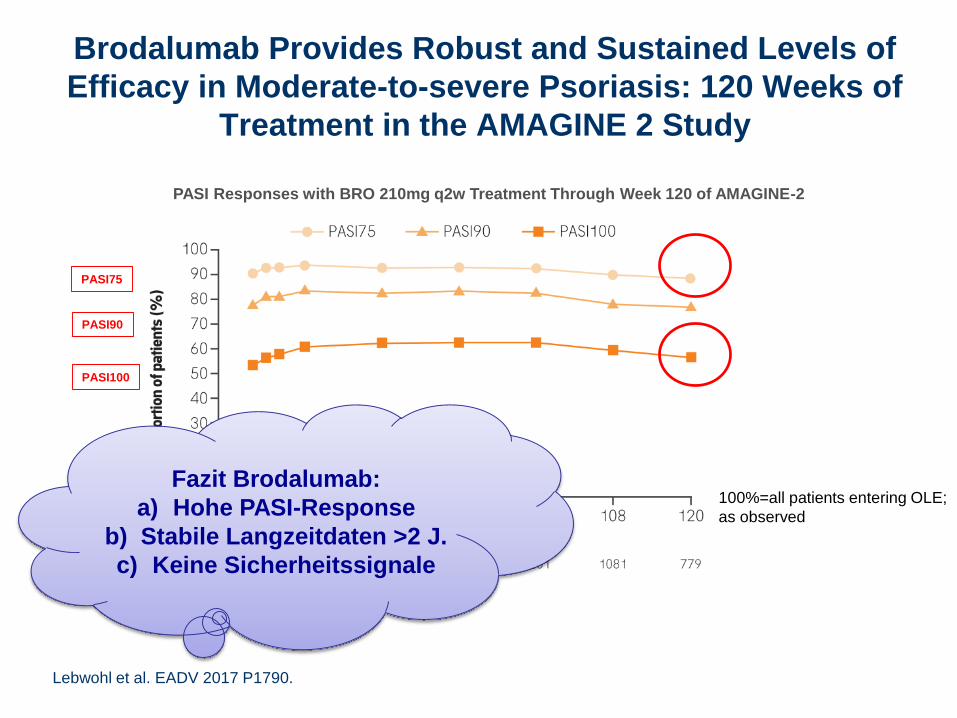
Brodalumab Provides Robust and Sustained Levels of
Efficacy in Moderate-to-severe Psoriasis: 120 Weeks of
Treatment in the AMAGINE 2 Study
PASI Responses with BRO 210mg q2w Treatment Through Week 120 of AMAGINE-2
100%=all patients entering OLE;
as observed
Lebwohl et al. EADV 2017 P1790.
PASI75
PASI90
PASI100
Brodalumab Provides Robust and Sustained Levels of
Efficacy in Moderate-to-severe Psoriasis: 120 Weeks of
Treatment in the AMAGINE 2 Study
PASI Responses with BRO 210mg q2w Treatment Through Week 120 of AMAGINE-2
100%=all patients entering OLE;
as observed
Lebwohl et al. EADV 2017 P1790.
PASI75
PASI90
PASI100
Fazit Brodalumab:
a) Hohe PASI-Response
b) Stabile Langzeitdaten >2 J.
c) Keine Sicherheitssignale
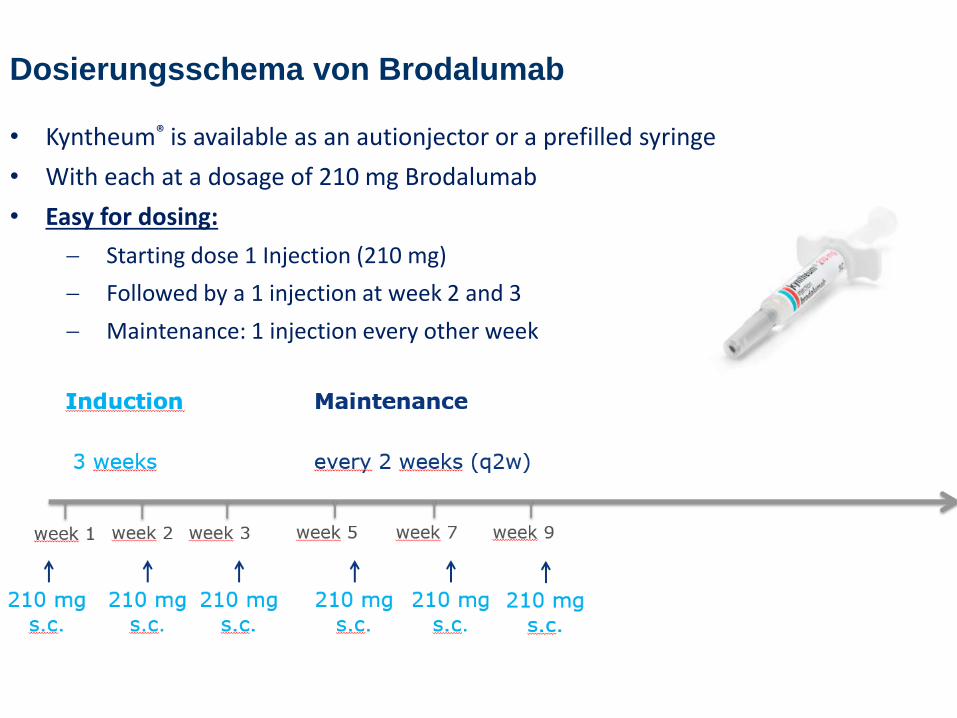
• Kyntheum® is available as an autionjector or a prefilled syringe
• With each at a dosage of 210 mg Brodalumab
• Easy for dosing:
Starting dose 1 Injection (210 mg)
Followed by a 1 injection at week 2 and 3
Maintenance: 1 injection every other week
Dosierungsschema von Brodalumab
IL-17 inhibition Immunogenität?
Overview of subjects with TE-AD-Ab in SKB Phase 3 studies in moderate to severe psoriasis
Subject/studySKB dose
(mg)Prior
biologic
Week of positive signal
AD-Ab (titer)
Neutralizing antibodies
Efficacy lossAE
possibly 1g related
PK
1/ERASURE 150 None 12 No titer* Yes No None Normal
2/ERASURE PBO 150 None 24No titer*
No No NoneNot
available
3/FIXTURE 150 None 24 6.41 No No None Normal
4/FIXTURE150
None 12 No titer* No No None Normal
5/SCULPTURE150
FlNone
2452
2.842.69
YesNo None Normal
6/SCULPTURE150
RANNone 52 1.05 Yes
Regained response on retreatment
NoneNot
available
7/SCULPTURE150
FlETN 12 No titer* Not available
Partial responder
None Normal
8/FIXTURE 300 None 12 1.50 No No None Normal
9/FIXTURE 300 None 24 No titer* No No None Normal
10/SCULPTURE300FI
None 24 No titer* Not available No None Normal
FI, fixed interval; RAN, retreatment as needed. *Titer could not be determined
Reich K, et al. Br J Dermatol. 2017; 176:752-758
Immunogenicity of Secukinumab
Overview of subjects with TE-AD-Ab in SKB Phase 3 studies in moderate to severe psoriasis
Subject/studySKB dose
(mg)Prior
biologic
Week of positive signal
AD-Ab (titer)
Neutralizing antibodies
Efficacy lossAE
possibly 1g related
PK
1/ERASURE 150 None 12 No titer* Yes No None Normal
2/ERASURE PBO 150 None 24No titer*
No No NoneNot
available
3/FIXTURE 150 None 24 6.41 No No None Normal
4/FIXTURE150
None 12 No titer* No No None Normal
5/SCULPTURE150
FlNone
2452
2.842.69
YesNo None Normal
6/SCULPTURE150
RANNone 52 1.05 Yes
Regained response on retreatment
NoneNot
available
7/SCULPTURE150
FlETN 12 No titer* Not available
Partial responder
None Normal
8/FIXTURE 300 None 12 1.50 No No None Normal
9/FIXTURE 300 None 24 No titer* No No None Normal
10/SCULPTURE300FI
None 24 No titer* Not available No None Normal
FI, fixed interval; RAN, retreatment as needed. *Titer could not be determined
Reich K, et al. Br J Dermatol. 2017; 176:752-758
Immunogenicity of Secukinumab
Fazit Immunogenität bei
anti-IL-17-Ak:
a) Funktionell nicht
bedeutend
b) beste Daten für
Secukinumab
Zusammenfassung: Status IL-17 inhibition
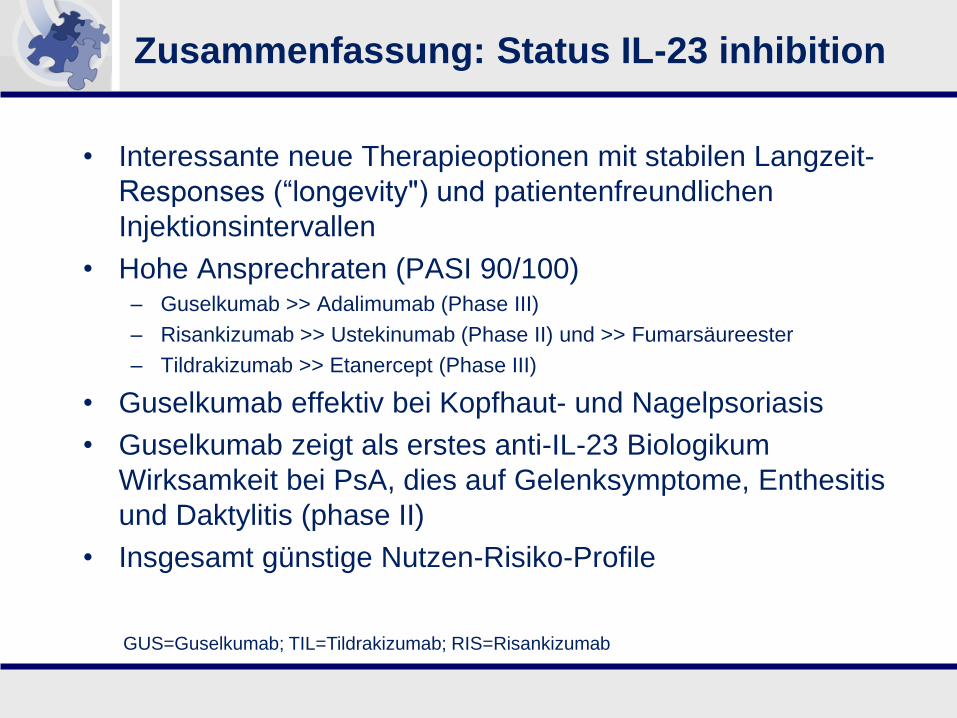
• EMA label: Secukinumab, Ixekizumab, Brodalumab
• Schnelle und hohe Response (PASI 90/100)– SEC>ETN, SEC>UST, IXE>ETN, IXE>UST, SEC>FAEs, IXE>FAEs, MTX
• Effektiv bei vielen Pso-Manifestationen (SEC; scalp, nails,
palmoplantar, PsA)
• Langzeit-Response bei allen 3 Präparaten
• Diskussion über “controlled disease/disease modification“ in
Subgruppe von Patienten
• Unterschiede in der klinisch relevanten Immunogenität?
• Erste Evidenz für potentiell kardioprotektiven Effekt (SEC)
1 SCIderm Research Institute and Dermatologikum Hamburg, Hamburg, Germany; 2K. Papp Clinical Research and
Probity Medical Research, Waterloo, Ontario, Canada; 3Oregon Medical Research Center, Portland, OR, USA; 4Department of Dermatology, University of Texas, Houston, TX, USA; 5University of Melbourne, Melbourne, VIC, Australia; 6University of Lübeck, Lübeck, Germany; 7Merck & Co., Inc., Kenilworth, NJ, USA
European Academy of Dermatology and Venereology, Output Size: 47.81” x 33.11” Scale: 200%
INTRODUCTION
• Tildrakizumab (TIL) is a high-affinity, humanized, IgG1/κ, anti-IL-23p19 monoclonal antibody under development for the treatment of moderate-to-severe chronic plaque psoriasis
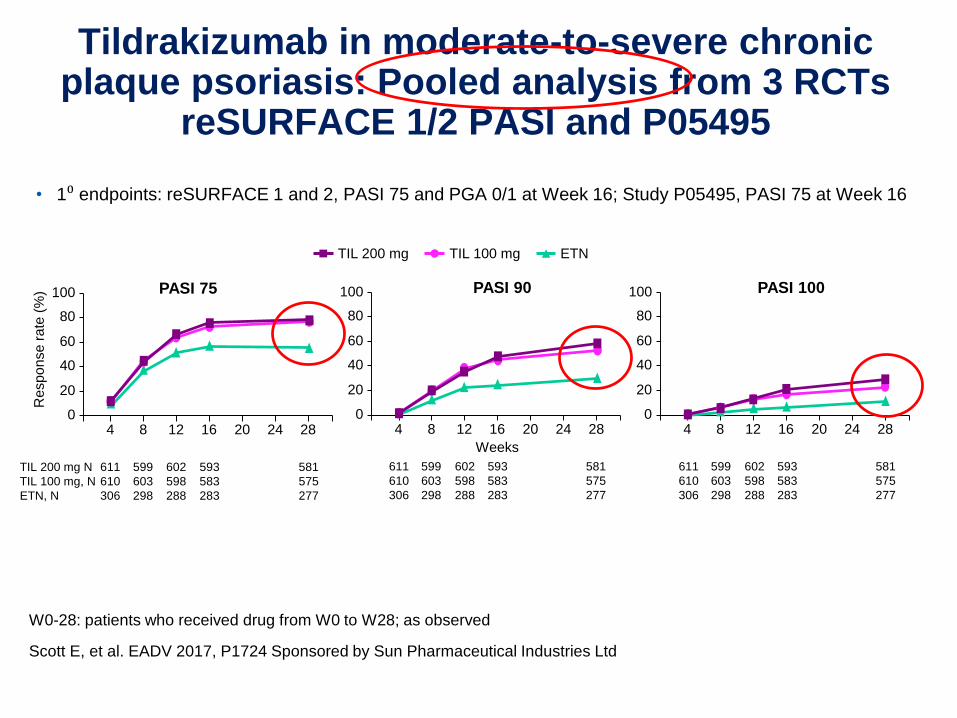
• TIL has been shown to result in significantly higher Psoriasis Area and Severity Index (PASI) 75, 90, and 100 and Physician’s Global Assessment (PGA) response rates compared with placebo1,2
• PASI and PGA are the most commonly used measures of psoriasis severity
• The association between PASI improvement and PGA response has not been investigated for treatment with TIL
OBJECTIVE
• To assess whether there was an association between PASI and PGA responses using data from two Phase 3 studies of TIL
MATERIALS & METHODS
• Two randomized controlled studies of TIL for chronic plaque psoriasis, reSURFACE 1 (Phase 3; NCT01722331) and reSURFACE 2 (Phase 3; NCT01729754), have been previously described2
• Patients in the studies were adults with moderate to severe plaque psoriasis, defined as ≥10% body surface area, ≥3 PGA, and PASI ≥12
• In Part 1 (weeks 1–12) of the studies, patients were randomized to subcutaneous TIL 200 mg, 100 mg, or placebo, and treatment was administered at weeks 0 and 4
– In reSURFACE 2, etanercept (ETN) 50 mg administered 2x/week was an additional treatment arm
• In Part 2 (weeks 12–28) of the studies, all patients receiving placebo in Part 1 were re-randomized to TIL 200 mg or 100 mg and received TIL at weeks 12, 16, and 28
– Patients receiving TIL in Part 1 continued their originally randomized treatment and received a dose of TIL at week 16
– Patients receiving ETN in Part 1 of reSURFACE 2 continued ETN, but administered 1x/week
• Co-primary endpoints in both studies were the proportion of patients achieving at least PASI 75 and the proportion achieving a PGA score of “clear” or “minimal,” with at least a 2-grade reduction from baseline (PGA response) at week 12
– The proportion achieving PASI 90 and 100 at week 12 were key secondary endpoints
– The proportion achieving PASI 75 and PGA score of ‘clear’ or ‘minimal’ with at least a 2-grade reduction from baseline (PGA response), at weeks 12 and 28 vs ETN were key secondary endpoints in reSURFACE 2
CONCLUSIONS
• There was a high and significant association between PASI 75, PASI 90, or PASI 100 responses and achieving PGA 0/1 in tildrakizumab studies at weeks 12 and 28 in patients with moderate-to-severe chronic plaque psoriasis
• PASI 100 is more strongly associated with PGA response than PASI 75 or PASI 90 in trials of TIL
References
1. Papp K, et al. Br J Dermatol. 2015;173(4):930-939.
2. Reich K, et al. Lancet. 2017;390(10091):276-288.
Disclosures
K. Reich has served as consultant and/or paid speaker for and/or participated in clinical trials sponsored by AbbVie, Amgen, Biogen Idec, Celgene, Centocor, Covagen, Forward Pharma, GlaxoSmithKline, Janssen-Cilag, Leo, Lilly, Medac, Merck & Co., Inc., Novartis, Pfizer, Vertex, and Takeda. K.A. Papp has provided professional services to AbbVie, Amgen, Anacor, Active Biotech, Allergan, Astellas, AstraZeneca, Basilea, Bayer, Biogen Idec, BMS, Boehringer Ingelheim, CanFite, Celgene, Coherus, Dermira, Eli Lilly, Forward Pharma, Genentech, GSK, Janssen, Kyowa Hako Kirin, Kythera, Leo Pharma, Merck Sharp & Dohme Corp., Merck-Serono, Novartis, Pfizer, Regeneron, Rigel, Roche, Sanofi-Genzyme, Sun Pharma, Takeda, UCB, Valeant, and Xenon. A. Blauvelt has served as a scientific adviser and clinical study investigator for AbbVie, Aclaris, Allergan, Almirall, Amgen, Boehringer Ingelheim, Celgene, Dermavant, Dermira, Eli Lilly and Company, Genentech/Roche, GlaxoSmithKline, Janssen, Leo, Merck & Co., Inc., Novartis, Pfizer, Purdue Pharma, Regeneron, Sandoz, Sanofi Genzyme, Sienna Pharmaceuticals, Sun Pharma, UCB, Valeant, and Vidac and as a paid speaker for Eli Lilly and Company, Janssen, Regeneron, and Sanofi Genzyme. S. Tyring has participated in trials supported by grants from Merck & Co., Inc., Kenilworth, NJ, USA. R. Sinclair has provided professional services to Leo Pharma, Amgen, Novartis, Merck & Co., Inc., Celgene, Coherus Biosciences, Janssen, Regeneron, MedImmune, GlaxoSmithKline, Cutanea, Samson Clinical, Boehringer Ingelheim, Pfizer, MSD, Oncobiologics, Roche, Eli Lilly and Company, and Bayer. D. Thaci has served as consultant, advisory board member, and/or investigator for AbbVie, Almiral, Amgen, Biogen Idec, Boehringer Ingelheim, Celgene, Dignity, Galderma, GlaxoSmithKline, Janssen-Cilag, Leo Pharma, Lilly, Maruho, Medac, MedImmune, MSD, Novartis, Regeneron, Sandoz, Sanofi-Aventis, Sun Pharma, Takeda, and Pfizer. Q. Li, N. Cichanowitz, S. Green, and C. La Rosa are employees of Merck & Co., Inc., Kenilworth, NJ, USA.
• The proportion of response was analyzed using the Cochran-Mantel-Haenszel test stratified by weight (≤90 kg, >90 kg) and prior exposure to biologics for psoriasis
• At week 12, analysis using nonresponder imputation was prespecified
• At week 28, analysis using nonresponder imputation was prespecified for PASI 75 and PGA response in reSURFACE 2; analysis of observed data was prespecified for PASI 75, 90, 100, and PGA response in reSURFACE 1 and for PASI 90 and 100 in reSURFACE 2
• Chi-square test was used on the odds ratio for the association between the proportion of PASI 75, PASI 90, or PASI 100 and PGA responders using pooled data from patients in all treatment groups who had both PASI and PGA assessments at baseline and weeks 12 or 28
• P-values were not adjusted for multiplicity
RESULTS
• In all, 772 patients were included in reSURFACE 1 and 1,090 patients were included in reSURFACE 2
• For reSURFACE 1/reSURFACE 2, PASI 75, 90, and 100 and PGA 0/1 response rates at week 12 with TIL 200 mg and 100 mg are shown in Figure 1
– Response rates at week 28 are shown in Figure 2
• Statistically significant associations between PASI 75, 90, and 100 responses and PGA 0/1 responses were observed at both weeks 12 and 28 (Table 1; P<0.001 for all associations)
• Interpretation of the odds ratios indicates that, for example, with an odds ratio of 47.0 for PASI 75 and PGA response at week 12, for a PASI 75 responder, the odds of getting a PGA response are ~47 times larger than the odds for a PASI 75 nonresponder
• Thus, based on the odds ratios, the association between PASI 100 and PGA response is higher than that of PASI 75 or PASI 90 and PGA response
• Although only 17.1% -23.7% of patients at week 12 were both PASI 100 and PGA responders, 76.3% -82.9% of patients were still PGA responders (Table 1)
• At week 28, 32.8%-40.8% were both PASI 100 and PGA responders; 59.2% -67.2% of patients were still PGA responders (Table 1)
Table 1. Association Between the Proportion of Patients With PASI and PGA Response at Weeks 12 and 28
PASI Response
reSURFACE 1 reSURFACE 2
PGA Response,% No
PGA Response,% Yes
Odds Ratio (95% CI) P-valuea
PGA Response,% No
PGA Response,% Yes
Odds Ratio (95% CI) P-valuea
Week 12 n=374 n=372 n=512 n=510
PASI 75 response
No 83.4 9.7 81.4 11.0
Yes 16.6 90.3 47.0 (30.3, 72.8)
<0.001 18.6 89.0 35.6 (24.9, 50.8)
<0.001
PASI 90 response
No 97.9 43.0 96.5 44.7
Yes 2.1 57.0 60.6 (29.2, 125.8)
<0.001 3.5 55.3 33.9 (20.6, 56.1)
<0.001
PASI 100 response
No 100 76.3 100 82.9
Yes 0 23.7 233.0 (14.4, 3770.3)
<0.001 0 17.1 211.8 (13.1, 3422.8)
<0.001
Week 28 n=186 n=387 n=326 n=528
PASI 75 response
No 51.1 3.4 69.0 8.3
Yes 48.9 96.6 30.0 (16.1, 56.0)
<0.001 31.0 91.7 24.5 (16.6, 36.1)
<0.001
PASI 90 response
No 86.0 24.8 93.3 26.1
Yes 14.0 75.2 18.7 (11.6, 30.0)
<0.001 6.7 73.9 39.1 (24.3, 62.8)
<0.001
PASI 100 response
No 100 59.2 100 67.2
Yes 0 40.8 257.6
(15.9, 4164.4)
<0.001 0 32.8 318.7
(19.8, 5136.3)
<0.001
PASI, Psoriasis Area and Severity Index; PGA, Physician’s Global Assessment.aP-values not adjusted for multiplicity.
Figure 1. PASI 75, 90, and 100 and PGA 0/1 Response
Rates With TIL in reSURFACE 1 and 2 at Week 12.
Nonresponder imputation was prespecified.
0
10
20
30
40
50
60
70
80
90
100
PASI 75 PASI 90 PASI 100 PGA 0/1
Resp
on
se R
ate
, %
reSURFACE 1: Week 12 TIL 200 mg
TIL 100 mg
0
10
20
30
40
50
60
70
80
90
100
PASI 75 PASI 90 PASI 100 PGA 0/1
Re
spo
nse R
ate
, %
reSURFACE 2: Week 12
62
35
14
5964
35
14
58
66
37
12
5961
39
12
55
PASI, Psoriasis Area and Severity Index; PGA, Physician’s Global Assessment; TIL, tildrakizumab.
Figure 2. PASI 75, 90, and 100 and PGA 0/1 Response
Rates With TIL in reSURFACE 1 and 2 at Week 28.
Nonresponder imputation was prespecified for PASI
75 and PGA in reSURFACE 2; analysis of observed
data was prespecified for all other endpoints shown.
82
59
32
69
80
52
24
66
0
10
20
30
40
50
60
70
80
90
100
PASI 75 PASI 90 PASI 100 PGA 0/1
Resp
onse
Rate
, %
reSURFACE 1: Week 28 TIL 200 mg
TIL 100 mg
73
58
27
6974
56
23
65
0
10
20
30
40
50
60
70
80
90
100
PASI 75 PASI 90 PASI 100 PGA 0/1
Resp
on
se R
ate
, %
reSURFACE 2: Week 28
PASI, Psoriasis Area and Severity Index; PGA, Physician’s Global Assessment; TIL, tildrakizumab.
1 SCIderm Research Institute and Dermatologikum Hamburg, Hamburg, Germany; 2K. Papp Clinical Research and
Probity Medical Research, Waterloo, Ontario, Canada; 3Oregon Medical Research Center, Portland, OR, USA; 4Department of Dermatology, University of Texas, Houston, TX, USA; 5University of Melbourne, Melbourne, VIC, Australia; 6University of Lübeck, Lübeck, Germany; 7Merck & Co., Inc., Kenilworth, NJ, USA
European Academy of Dermatology and Venereology, Output Size: 47.81” x 33.11” Scale: 200%
INTRODUCTION
• Tildrakizumab (TIL) is a high-affinity, humanized, IgG1/κ, anti-IL-23p19 monoclonal antibody under development for the treatment of moderate-to-severe chronic plaque psoriasis
• TIL has been shown to result in significantly higher Psoriasis Area and Severity Index (PASI) 75, 90, and 100 and Physician’s Global Assessment (PGA) response rates compared with placebo1,2
• PASI and PGA are the most commonly used measures of psoriasis severity
• The association between PASI improvement and PGA response has not been investigated for treatment with TIL
OBJECTIVE
• To assess whether there was an association between PASI and PGA responses using data from two Phase 3 studies of TIL
MATERIALS & METHODS
• Two randomized controlled studies of TIL for chronic plaque psoriasis, reSURFACE 1 (Phase 3; NCT01722331) and reSURFACE 2 (Phase 3; NCT01729754), have been previously described2
• Patients in the studies were adults with moderate to severe plaque psoriasis, defined as ≥10% body surface area, ≥3 PGA, and PASI ≥12
• In Part 1 (weeks 1–12) of the studies, patients were randomized to subcutaneous TIL 200 mg, 100 mg, or placebo, and treatment was administered at weeks 0 and 4
– In reSURFACE 2, etanercept (ETN) 50 mg administered 2x/week was an additional treatment arm
• In Part 2 (weeks 12–28) of the studies, all patients receiving placebo in Part 1 were re-randomized to TIL 200 mg or 100 mg and received TIL at weeks 12, 16, and 28
– Patients receiving TIL in Part 1 continued their originally randomized treatment and received a dose of TIL at week 16
– Patients receiving ETN in Part 1 of reSURFACE 2 continued ETN, but administered 1x/week
• Co-primary endpoints in both studies were the proportion of patients achieving at least PASI 75 and the proportion achieving a PGA score of “clear” or “minimal,” with at least a 2-grade reduction from baseline (PGA response) at week 12
– The proportion achieving PASI 90 and 100 at week 12 were key secondary endpoints
– The proportion achieving PASI 75 and PGA score of ‘clear’ or ‘minimal’ with at least a 2-grade reduction from baseline (PGA response), at weeks 12 and 28 vs ETN were key secondary endpoints in reSURFACE 2
CONCLUSIONS
• There was a high and significant association between PASI 75, PASI 90, or PASI 100 responses and achieving PGA 0/1 in tildrakizumab studies at weeks 12 and 28 in patients with moderate-to-severe chronic plaque psoriasis
• PASI 100 is more strongly associated with PGA response than PASI 75 or PASI 90 in trials of TIL
References
1. Papp K, et al. Br J Dermatol. 2015;173(4):930-939.
2. Reich K, et al. Lancet. 2017;390(10091):276-288.
Disclosures
K. Reich has served as consultant and/or paid speaker for and/or participated in clinical trials sponsored by AbbVie, Amgen, Biogen Idec, Celgene, Centocor, Covagen, Forward Pharma, GlaxoSmithKline, Janssen-Cilag, Leo, Lilly, Medac, Merck & Co., Inc., Novartis, Pfizer, Vertex, and Takeda. K.A. Papp has provided professional services to AbbVie, Amgen, Anacor, Active Biotech, Allergan, Astellas, AstraZeneca, Basilea, Bayer, Biogen Idec, BMS, Boehringer Ingelheim, CanFite, Celgene, Coherus, Dermira, Eli Lilly, Forward Pharma, Genentech, GSK, Janssen, Kyowa Hako Kirin, Kythera, Leo Pharma, Merck Sharp & Dohme Corp., Merck-Serono, Novartis, Pfizer, Regeneron, Rigel, Roche, Sanofi-Genzyme, Sun Pharma, Takeda, UCB, Valeant, and Xenon. A. Blauvelt has served as a scientific adviser and clinical study investigator for AbbVie, Aclaris, Allergan, Almirall, Amgen, Boehringer Ingelheim, Celgene, Dermavant, Dermira, Eli Lilly and Company, Genentech/Roche, GlaxoSmithKline, Janssen, Leo, Merck & Co., Inc., Novartis, Pfizer, Purdue Pharma, Regeneron, Sandoz, Sanofi Genzyme, Sienna Pharmaceuticals, Sun Pharma, UCB, Valeant, and Vidac and as a paid speaker for Eli Lilly and Company, Janssen, Regeneron, and Sanofi Genzyme. S. Tyring has participated in trials supported by grants from Merck & Co., Inc., Kenilworth, NJ, USA. R. Sinclair has provided professional services to Leo Pharma, Amgen, Novartis, Merck & Co., Inc., Celgene, Coherus Biosciences, Janssen, Regeneron, MedImmune, GlaxoSmithKline, Cutanea, Samson Clinical, Boehringer Ingelheim, Pfizer, MSD, Oncobiologics, Roche, Eli Lilly and Company, and Bayer. D. Thaci has served as consultant, advisory board member, and/or investigator for AbbVie, Almiral, Amgen, Biogen Idec, Boehringer Ingelheim, Celgene, Dignity, Galderma, GlaxoSmithKline, Janssen-Cilag, Leo Pharma, Lilly, Maruho, Medac, MedImmune, MSD, Novartis, Regeneron, Sandoz, Sanofi-Aventis, Sun Pharma, Takeda, and Pfizer. Q. Li, N. Cichanowitz, S. Green, and C. La Rosa are employees of Merck & Co., Inc., Kenilworth, NJ, USA.
• The proportion of response was analyzed using the Cochran-Mantel-Haenszel test stratified by weight (≤90 kg, >90 kg) and prior exposure to biologics for psoriasis
• At week 12, analysis using nonresponder imputation was prespecified
• At week 28, analysis using nonresponder imputation was prespecified for PASI 75 and PGA response in reSURFACE 2; analysis of observed data was prespecified for PASI 75, 90, 100, and PGA response in reSURFACE 1 and for PASI 90 and 100 in reSURFACE 2
• Chi-square test was used on the odds ratio for the association between the proportion of PASI 75, PASI 90, or PASI 100 and PGA responders using pooled data from patients in all treatment groups who had both PASI and PGA assessments at baseline and weeks 12 or 28
• P-values were not adjusted for multiplicity
RESULTS
• In all, 772 patients were included in reSURFACE 1 and 1,090 patients were included in reSURFACE 2
• For reSURFACE 1/reSURFACE 2, PASI 75, 90, and 100 and PGA 0/1 response rates at week 12 with TIL 200 mg and 100 mg are shown in Figure 1
– Response rates at week 28 are shown in Figure 2
• Statistically significant associations between PASI 75, 90, and 100 responses and PGA 0/1 responses were observed at both weeks 12 and 28 (Table 1; P<0.001 for all associations)
• Interpretation of the odds ratios indicates that, for example, with an odds ratio of 47.0 for PASI 75 and PGA response at week 12, for a PASI 75 responder, the odds of getting a PGA response are ~47 times larger than the odds for a PASI 75 nonresponder
• Thus, based on the odds ratios, the association between PASI 100 and PGA response is higher than that of PASI 75 or PASI 90 and PGA response
• Although only 17.1% -23.7% of patients at week 12 were both PASI 100 and PGA responders, 76.3% -82.9% of patients were still PGA responders (Table 1)
• At week 28, 32.8%-40.8% were both PASI 100 and PGA responders; 59.2% -67.2% of patients were still PGA responders (Table 1)
Table 1. Association Between the Proportion of Patients With PASI and PGA Response at Weeks 12 and 28
PASI Response
reSURFACE 1 reSURFACE 2
PGA Response,% No
PGA Response,% Yes
Odds Ratio (95% CI) P-valuea
PGA Response,% No
PGA Response,% Yes
Odds Ratio (95% CI) P-valuea
Week 12 n=374 n=372 n=512 n=510
PASI 75 response
No 83.4 9.7 81.4 11.0
Yes 16.6 90.3 47.0 (30.3, 72.8)
<0.001 18.6 89.0 35.6 (24.9, 50.8)
<0.001
PASI 90 response
No 97.9 43.0 96.5 44.7
Yes 2.1 57.0 60.6 (29.2, 125.8)
<0.001 3.5 55.3 33.9 (20.6, 56.1)
<0.001
PASI 100 response
No 100 76.3 100 82.9
Yes 0 23.7 233.0 (14.4, 3770.3)
<0.001 0 17.1 211.8 (13.1, 3422.8)
<0.001
Week 28 n=186 n=387 n=326 n=528
PASI 75 response
No 51.1 3.4 69.0 8.3
Yes 48.9 96.6 30.0 (16.1, 56.0)
<0.001 31.0 91.7 24.5 (16.6, 36.1)
<0.001
PASI 90 response
No 86.0 24.8 93.3 26.1
Yes 14.0 75.2 18.7 (11.6, 30.0)
<0.001 6.7 73.9 39.1 (24.3, 62.8)
<0.001
PASI 100 response
No 100 59.2 100 67.2
Yes 0 40.8 257.6
(15.9, 4164.4)
<0.001 0 32.8 318.7
(19.8, 5136.3)
<0.001
PASI, Psoriasis Area and Severity Index; PGA, Physician’s Global Assessment.aP-values not adjusted for multiplicity.
Figure 1. PASI 75, 90, and 100 and PGA 0/1 Response
Rates With TIL in reSURFACE 1 and 2 at Week 12.
Nonresponder imputation was prespecified.
0
10
20
30
40
50
60
70
80
90
100
PASI 75 PASI 90 PASI 100 PGA 0/1
Re
spo
nse R
ate
, %
reSURFACE 1: Week 12 TIL 200 mg
TIL 100 mg
0
10
20
30
40
50
60
70
80
90
100
PASI 75 PASI 90 PASI 100 PGA 0/1
Respo
nse
Rate
, %
reSURFACE 2: Week 12
62
35
14
5964
35
14
58
66
37
12
5961
39
12
55
PASI, Psoriasis Area and Severity Index; PGA, Physician’s Global Assessment; TIL, tildrakizumab.
Figure 2. PASI 75, 90, and 100 and PGA 0/1 Response
Rates With TIL in reSURFACE 1 and 2 at Week 28.
Nonresponder imputation was prespecified for PASI
75 and PGA in reSURFACE 2; analysis of observed
data was prespecified for all other endpoints shown.
82
59
32
69
80
52
24
66
0
10
20
30
40
50
60
70
80
90
100
PASI 75 PASI 90 PASI 100 PGA 0/1
Resp
on
se R
ate
, %
reSURFACE 1: Week 28 TIL 200 mg
TIL 100 mg
73
58
27
6974
56
23
65
0
10
20
30
40
50
60
70
80
90
100
PASI 75 PASI 90 PASI 100 PGA 0/1
Re
spo
nse
Rate
, %
reSURFACE 2: Week 28
PASI, Psoriasis Area and Severity Index; PGA, Physician’s Global Assessment; TIL, tildrakizumab.
Efficacy of Systemic Treatments for Moderate to Severe Plaque Psoriasis: Systematic Review and Meta-Analysis
Introduction Key Words
Abstract
Aims:
Methods:
Results:
Conclusions:
Do
wnlo
ad
ed b
y:
Sta
ats
- und
Univ
ers
itäts
bib
lioth
ek H
am
burg
13
4.1
00
.102
.2 -
10
/11/2
01
8 2
:56
:32 P
M
Comparative Effectiveness Research (CER) and
Network meta-analyses (NMA) in psoriasis
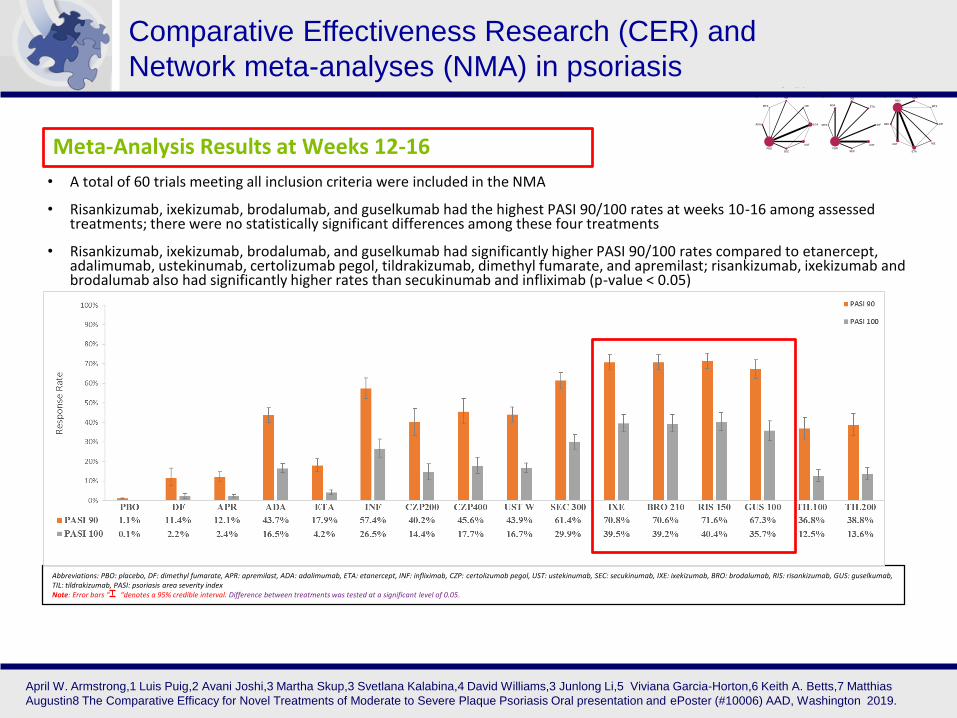
• A total of 60 trials meeting all inclusion criteria were included in the NMA
• Risankizumab, ixekizumab, brodalumab, and guselkumab had the highest PASI 90/100 rates at weeks 10-16 among assessed treatments; there were no statistically significant differences among these four treatments
• Risankizumab, ixekizumab, brodalumab, and guselkumab had significantly higher PASI 90/100 rates compared to etanercept, adalimumab, ustekinumab, certolizumab pegol, tildrakizumab, dimethyl fumarate, and apremilast; risankizumab, ixekizumab and brodalumab also had significantly higher rates than secukinumab and infliximab (p-value < 0.05)
Abbreviations: PBO: placebo, DF: dimethyl fumarate, APR: apremilast, ADA: adalimumab, ETA: etanercept, INF: infliximab, CZP: certolizumab pegol, UST: ustekinumab, SEC: secukinumab, IXE: ixekizumab, BRO: brodalumab, RIS: risankizumab, GUS: guselkumab, TIL: tildrakizumab, PASI: psoriasis area severity index Note: Error bars “ “denotes a 95% credible interval. Difference between treatments was tested at a significant level of 0.05.
Meta-Analysis Results at Weeks 12-16
April W. Armstrong,1 Luis Puig,2 Avani Joshi,3 Martha Skup,3 Svetlana Kalabina,4 David Williams,3 Junlong Li,5 Viviana Garcia-Horton,6 Keith A. Betts,7 Matthias
Augustin8 The Comparative Efficacy for Novel Treatments of Moderate to Severe Plaque Psoriasis Oral presentation and ePoster (#10006) AAD, Washington 2019.
Comparative Effectiveness Research (CER) and
Network meta-analyses (NMA) in psoriasis
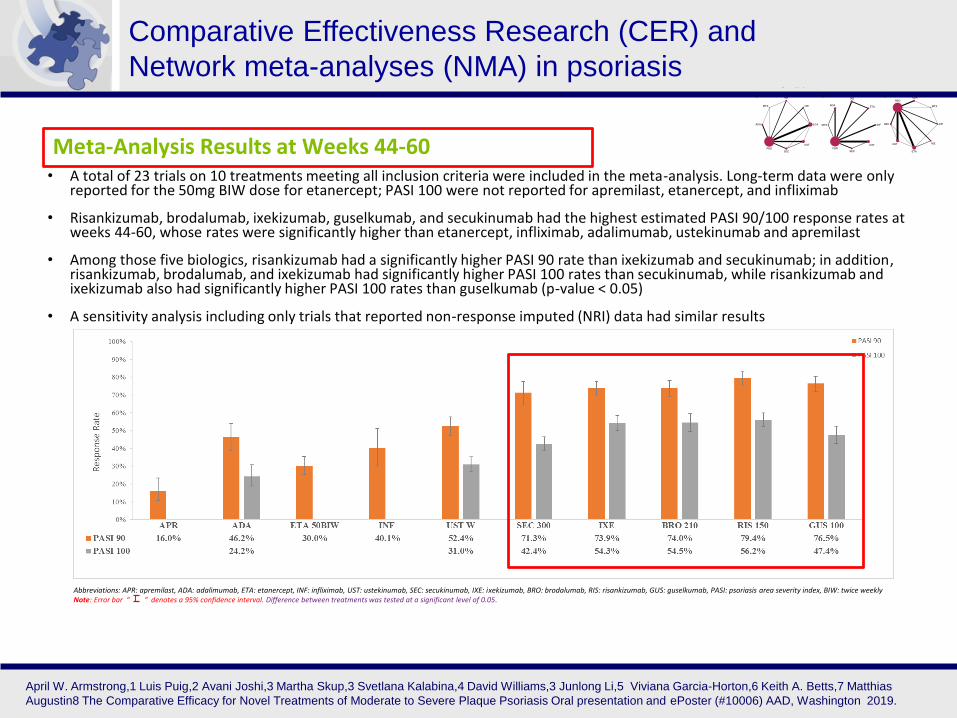
Meta-Analysis Results at Weeks 44-60• A total of 23 trials on 10 treatments meeting all inclusion criteria were included in the meta-analysis. Long-term data were only
reported for the 50mg BIW dose for etanercept; PASI 100 were not reported for apremilast, etanercept, and infliximab
• Risankizumab, brodalumab, ixekizumab, guselkumab, and secukinumab had the highest estimated PASI 90/100 response rates at weeks 44-60, whose rates were significantly higher than etanercept, infliximab, adalimumab, ustekinumab and apremilast
• Among those five biologics, risankizumab had a significantly higher PASI 90 rate than ixekizumab and secukinumab; in addition, risankizumab, brodalumab, and ixekizumab had significantly higher PASI 100 rates than secukinumab, while risankizumab and ixekizumab also had significantly higher PASI 100 rates than guselkumab (p-value < 0.05)
• A sensitivity analysis including only trials that reported non-response imputed (NRI) data had similar results
Abbreviations: APR: apremilast, ADA: adalimumab, ETA: etanercept, INF: infliximab, UST: ustekinumab, SEC: secukinumab, IXE: ixekizumab, BRO: brodalumab, RIS: risankizumab, GUS: guselkumab, PASI: psoriasis area severity index, BIW: twice weeklyNote: Error bar “ “ denotes a 95% confidence interval. Difference between treatments was tested at a significant level of 0.05.
April W. Armstrong,1 Luis Puig,2 Avani Joshi,3 Martha Skup,3 Svetlana Kalabina,4 David Williams,3 Junlong Li,5 Viviana Garcia-Horton,6 Keith A. Betts,7 Matthias
Augustin8 The Comparative Efficacy for Novel Treatments of Moderate to Severe Plaque Psoriasis Oral presentation and ePoster (#10006) AAD, Washington 2019.
Fazit für die Praxis
Biologika bei PSoriasis
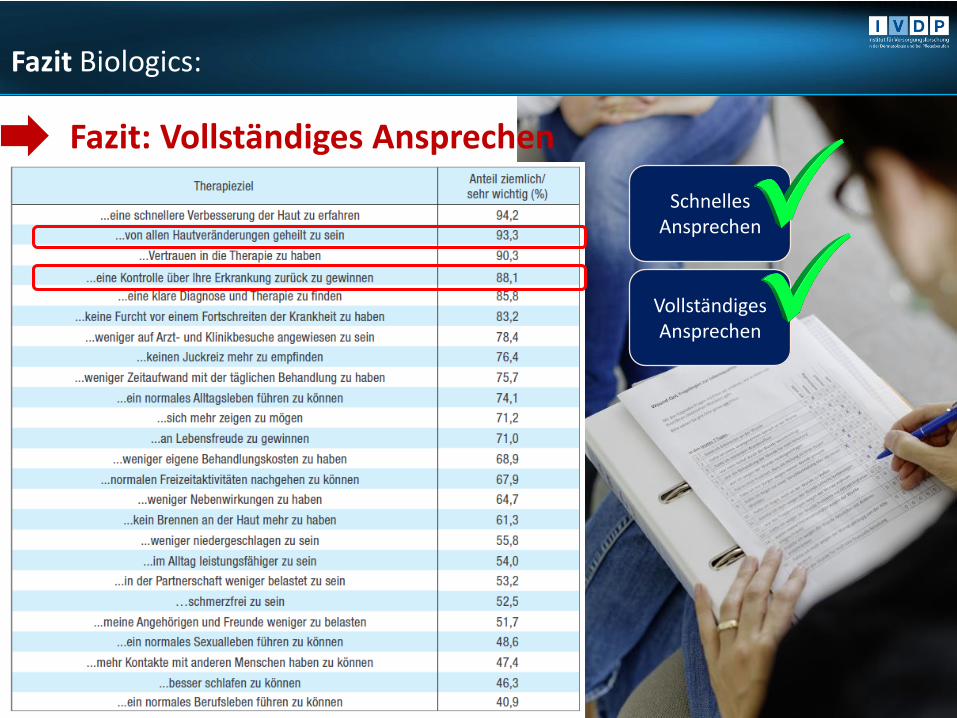
Fazit Biologics:
Fazit: Schnelles und langfristiges Ansprechen
Schnelles Ansprechen
Fazit: Vollständiges Ansprechen
Schnelles Ansprechen
Vollständiges Ansprechen
Fazit Biologics:
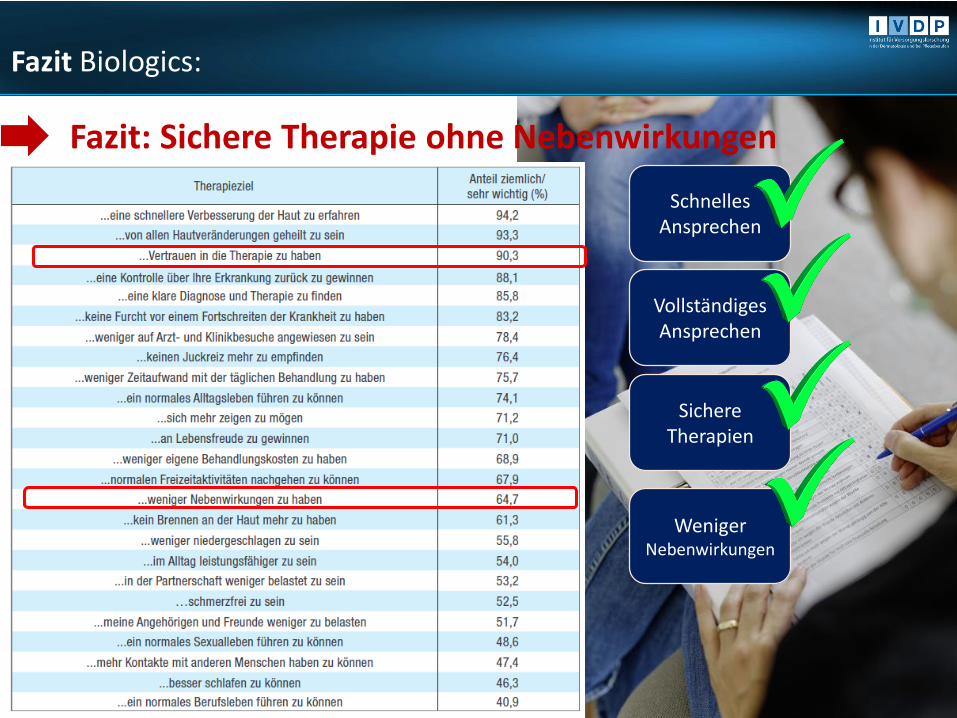
Fazit: Sichere Therapie ohne Nebenwirkungen Nebenwirkungen
Schnelles Ansprechen
Vollständiges Ansprechen
Sichere Therapien
Weniger Nebenwirkungen
Fazit Biologics:
Fazit: Weniger Zeitaufwand
Schnelles Ansprechen
Vollständiges Ansprechen
Sichere Therapien
Weniger Nebenwirkungen
Weniger Zeitaufwand
Fazit Biologics:
Herzlichen Dank für die
Aufmerksamkeit!
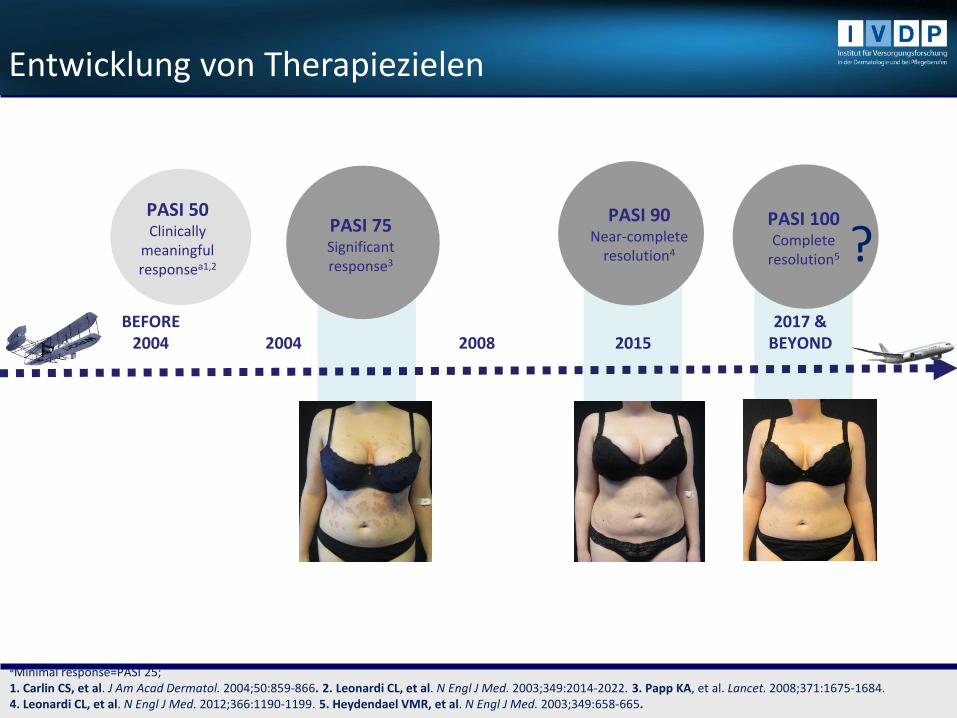
BEFORE 2004 2004 2008 2015
PASI 90Near-complete
resolution4
PASI 50Clinically
meaningfulresponsea1,2
PASI 100Complete
resolution5
2017 & BEYOND
PASI 75Significant response3
aMinimal response=PASI 25;1. Carlin CS, et al. J Am Acad Dermatol. 2004;50:859-866. 2. Leonardi CL, et al. N Engl J Med. 2003;349:2014-2022. 3. Papp KA, et al. Lancet. 2008;371:1675-1684. 4. Leonardi CL, et al. N Engl J Med. 2012;366:1190-1199. 5. Heydendael VMR, et al. N Engl J Med. 2003;349:658-665.
Entwicklung von Therapiezielen
?
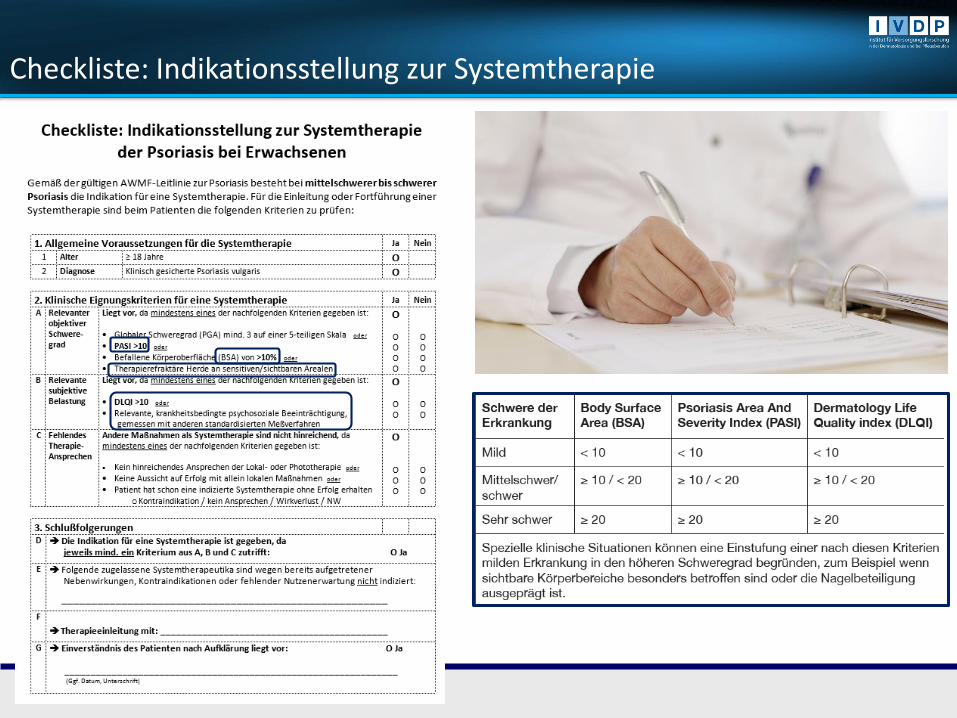
Checkliste: Indikationsstellung zur Systemtherapie