71
Herztransplantation Otmar Pfister Kardiologie
| Date post: | 19-Aug-2019 |
| Category: |
Documents |
| Upload: | truongkhanh |
| View: | 214 times |
| Download: | 0 times |

Herztransplantation
Otmar Pfister
Kardiologie
Christiaan Barnard, Cape Town
South Africa
Norman Shumway, Stanford, USA
Erste Herztransplantation: 3. Dezember 1967

Titel/Anlass/Autor

Zahlen
Patienten Selektion
Prätransplant. Abklärungen
Transplantation / frühe Post-Transplant Phase
Immunsuppression
Komplikationen
Posttransplant Nachsorge
Agenda
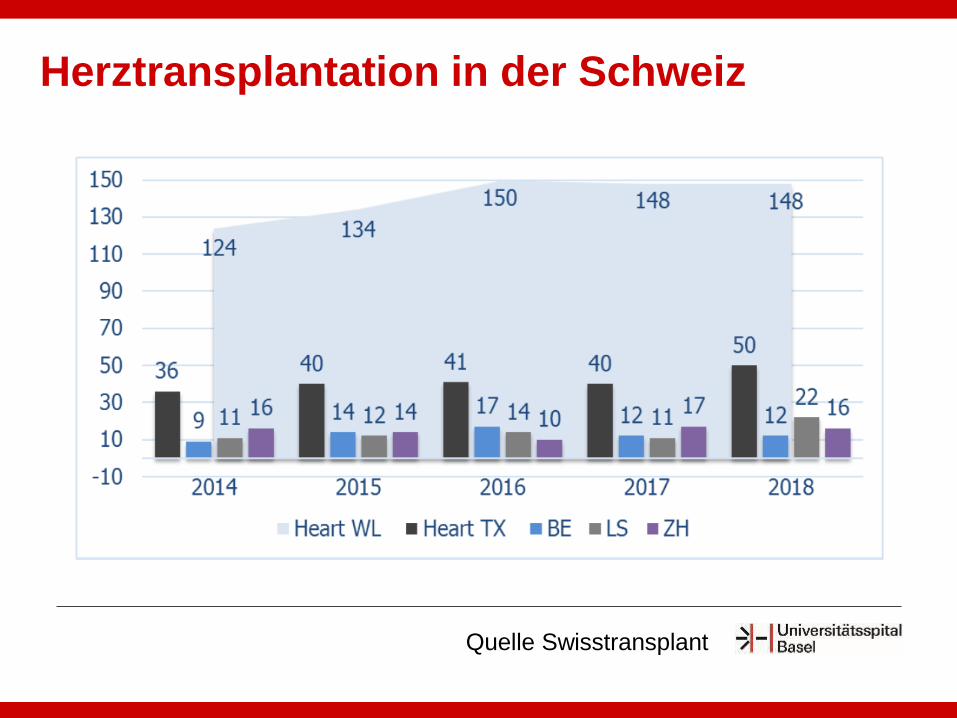
Herztransplantation in der Schweiz
Quelle Swisstransplant
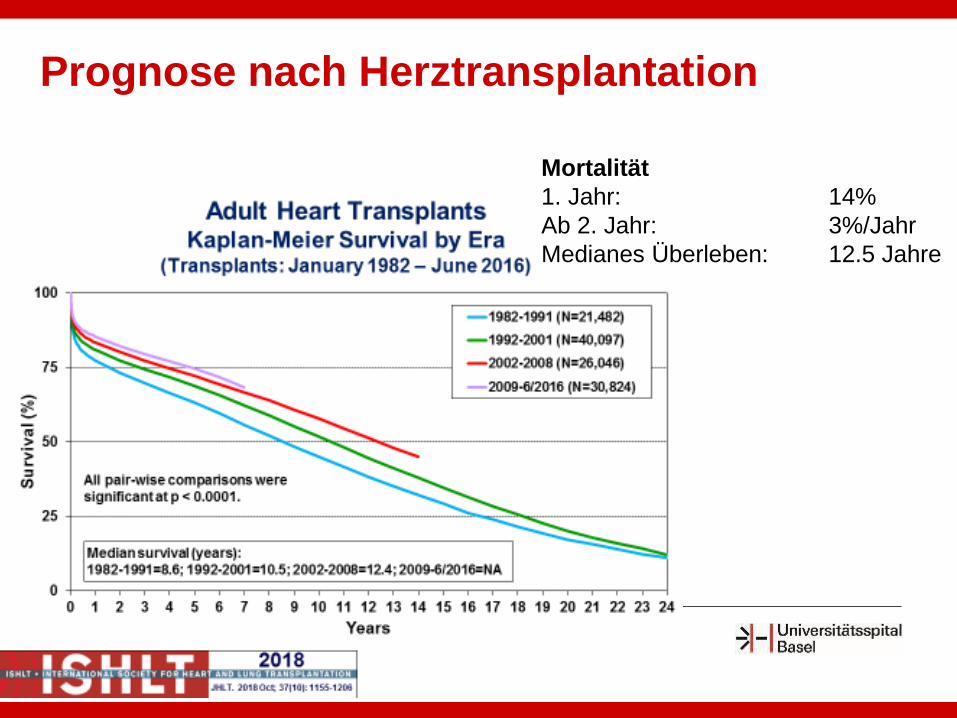
Prognose nach Herztransplantation
Mortalität
1. Jahr: 14%
Ab 2. Jahr: 3%/Jahr
Medianes Überleben: 12.5 Jahre
Aktuelle Kohorte: 26 Pat
HTx in Basel: 8
HTx in Zürich: 7
HTx in Bern: 11
HTx in Berlin: 1
Aktuelle HTx Kohorte Basel
Alter: 61 (29/83)
Frauen: 7 (27%)
Follow up (Jahre, median): 17 (1 – 34)
Diagnosen:
Frau A, 59 jährig
Wann listen?
Geschätzte Mortalität > 20% / Jahr• objektive Einschätzung schwierig
Möglichkeiten zur Risikostratifizierung
• Maximale Sauerstoffaufnahme (V02 max in
Spiroergometrie)
• „Aaronson-Mancini-Score“ (Heart Failure Survival
Score, HFSS)
• Seattle Heart Failure Model
• BNP (nicht etabliert)
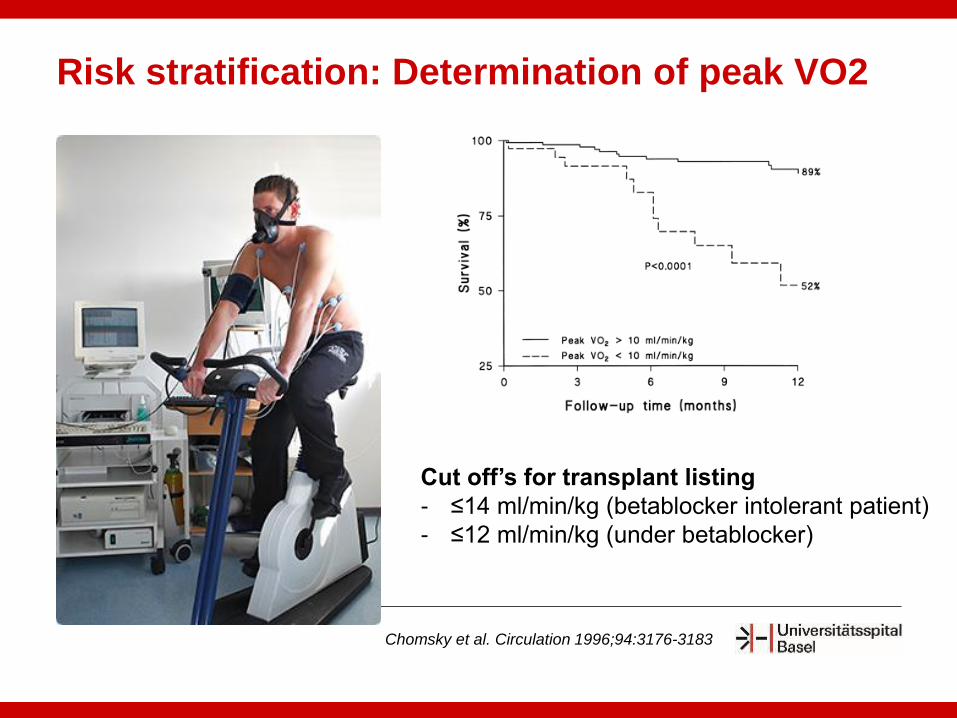
Chomsky et al. Circulation 1996;94:3176-3183
Risk stratification: Determination of peak VO2
Cut off’s for transplant listing
- ≤14 ml/min/kg (betablocker intolerant patient)
- ≤12 ml/min/kg (under betablocker)
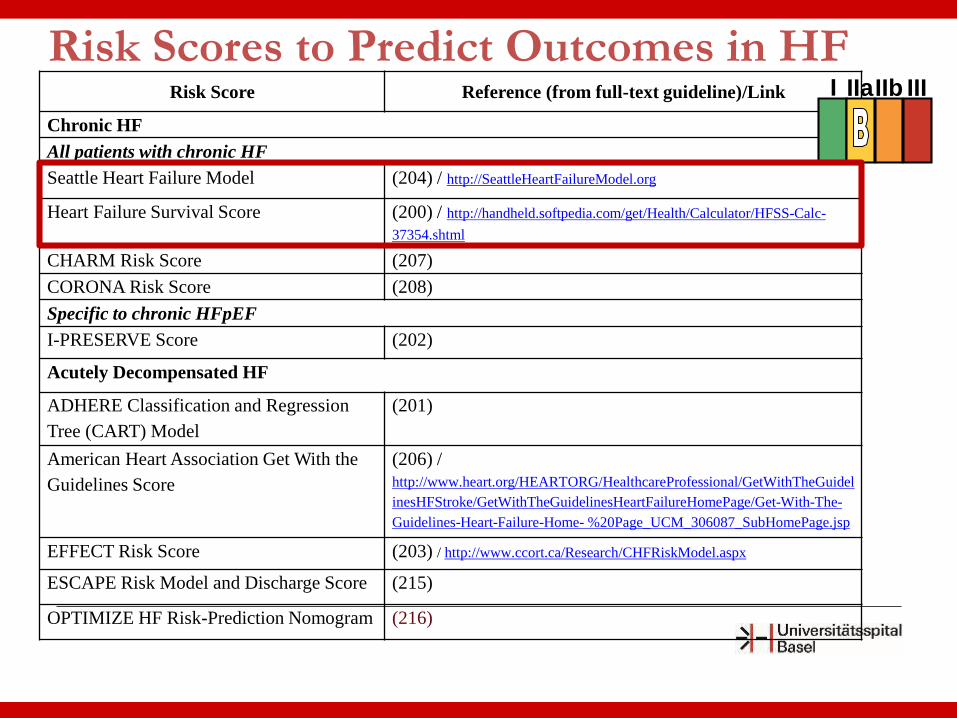
Risk Scores to Predict Outcomes in HFRisk Score Reference (from full-text guideline)/Link
Chronic HF
All patients with chronic HF
Seattle Heart Failure Model (204) / http://SeattleHeartFailureModel.org
Heart Failure Survival Score (200) / http://handheld.softpedia.com/get/Health/Calculator/HFSS-Calc-
37354.shtml
CHARM Risk Score (207)
CORONA Risk Score (208)
Specific to chronic HFpEF
I-PRESERVE Score (202)
Acutely Decompensated HF
ADHERE Classification and Regression
Tree (CART) Model
(201)
American Heart Association Get With the
Guidelines Score
(206) /
http://www.heart.org/HEARTORG/HealthcareProfessional/GetWithTheGuidel
inesHFStroke/GetWithTheGuidelinesHeartFailureHomePage/Get-With-The-
Guidelines-Heart-Failure-Home- %20Page_UCM_306087_SubHomePage.jsp
EFFECT Risk Score (203) / http://www.ccort.ca/Research/CHFRiskModel.aspx
ESCAPE Risk Model and Discharge Score (215)
OPTIMIZE HF Risk-Prediction Nomogram (216)
I IIaIIb III
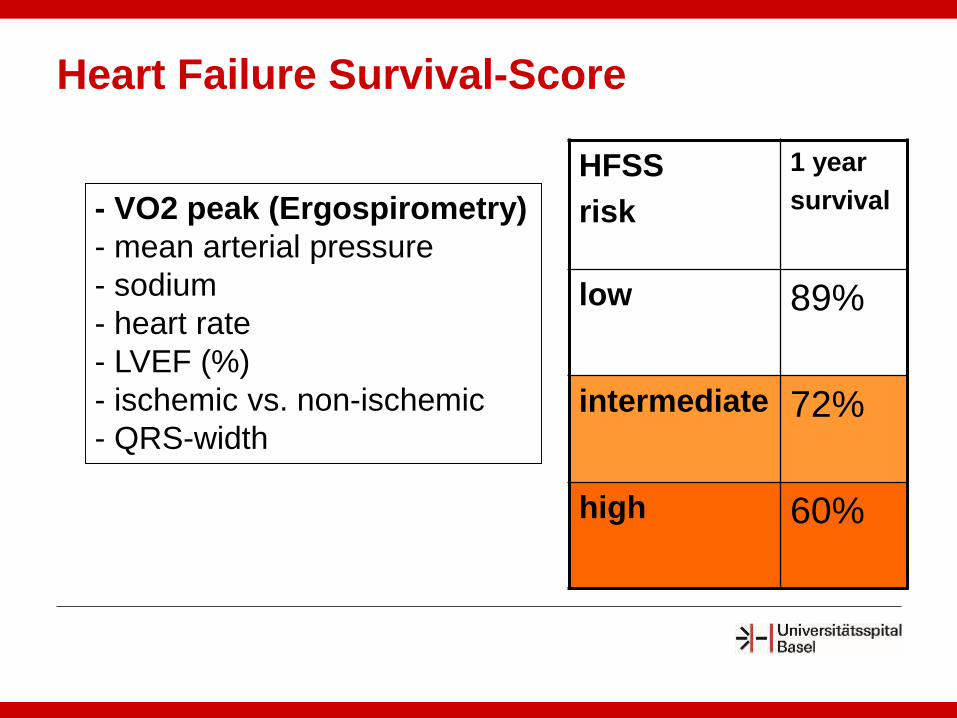
- VO2 peak (Ergospirometry)
- mean arterial pressure
- sodium
- heart rate
- LVEF (%)
- ischemic vs. non-ischemic
- QRS-width
HFSS
risk
1 year
survival
low 89%
intermediate 72%
high 60%
Heart Failure Survival-Score
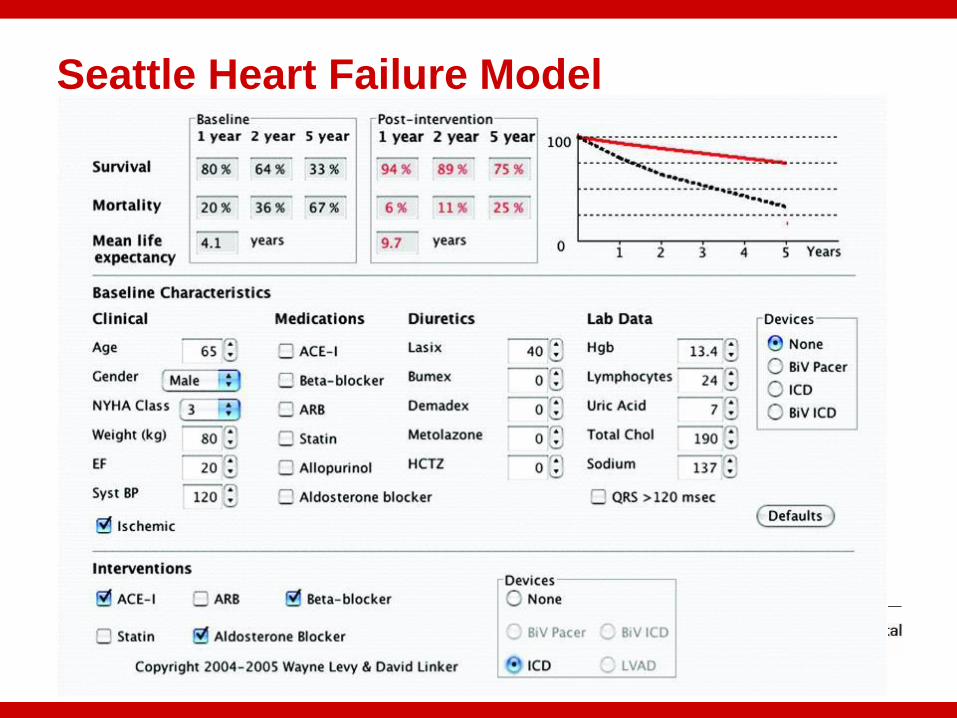
Seattle Heart Failure Model
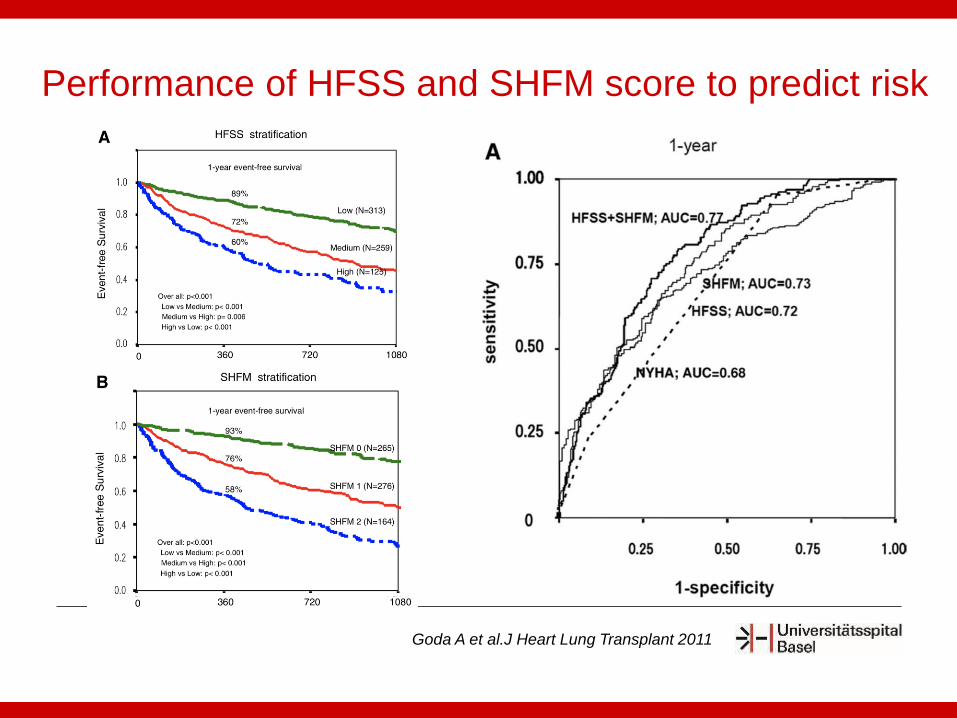
Performance of HFSS and SHFM score to predict risk
Goda A et al.J Heart Lung Transplant 2011
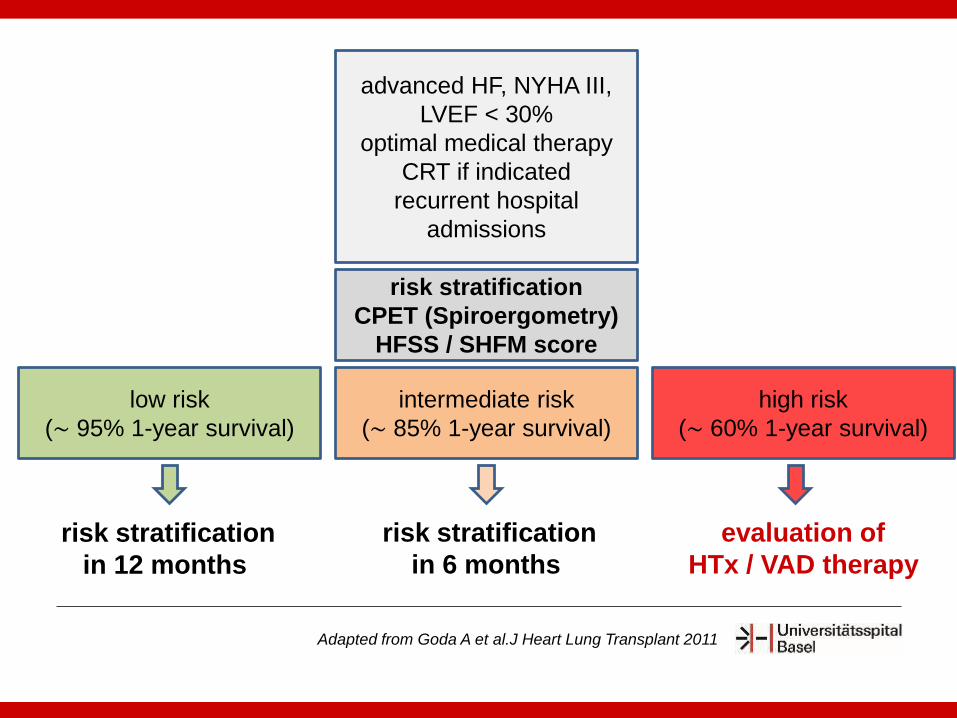
advanced HF, NYHA III,
LVEF < 30%
optimal medical therapy
CRT if indicated
recurrent hospital
admissions
risk stratification
CPET (Spiroergometry)
HFSS / SHFM score
low risk
(∼ 95% 1-year survival)
intermediate risk
(∼ 85% 1-year survival)
high risk
(∼ 60% 1-year survival)
risk stratification
in 12 months
risk stratification
in 6 months
evaluation of
HTx / VAD therapy
Adapted from Goda A et al.J Heart Lung Transplant 2011
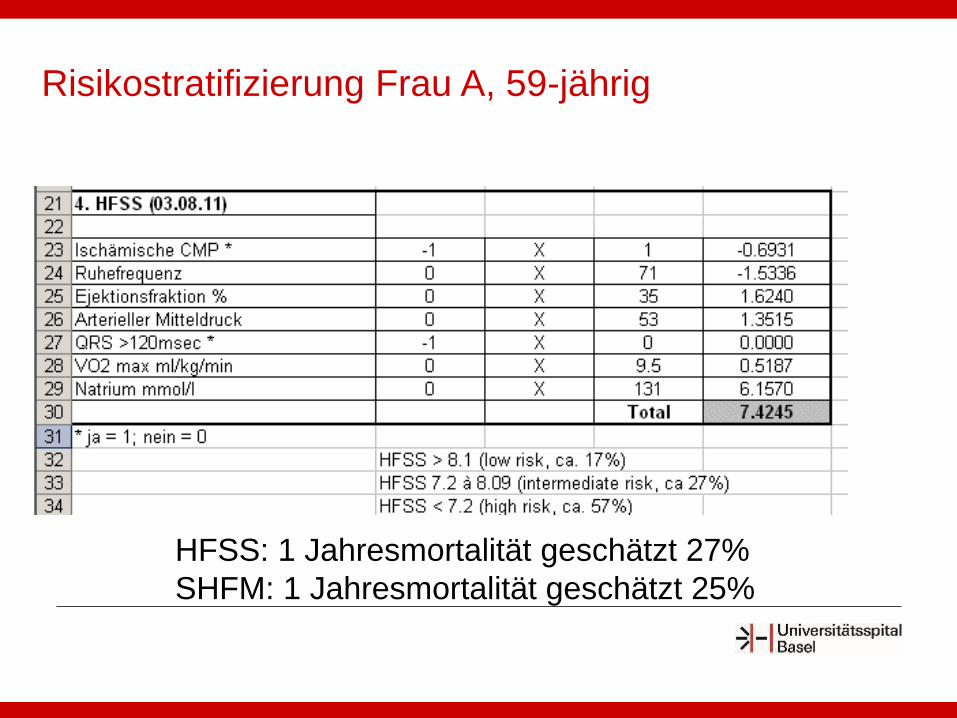
HFSS: 1 Jahresmortalität geschätzt 27%
SHFM: 1 Jahresmortalität geschätzt 25%
Risikostratifizierung Frau A, 59-jährig
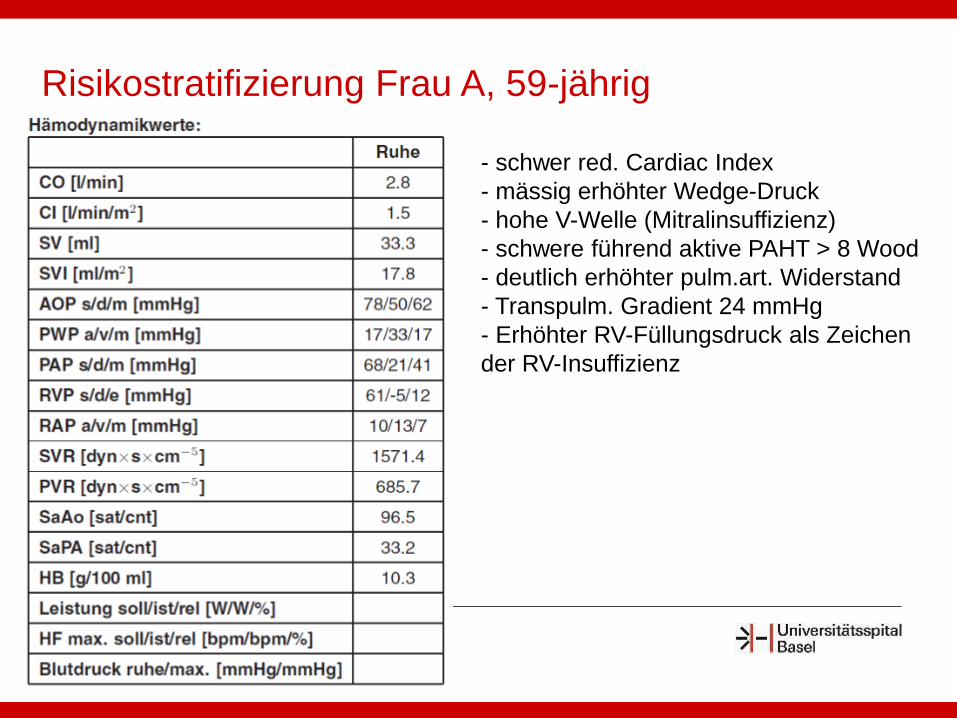
- schwer red. Cardiac Index
- mässig erhöhter Wedge-Druck
- hohe V-Welle (Mitralinsuffizienz)
- schwere führend aktive PAHT > 8 Wood
- deutlich erhöhter pulm.art. Widerstand
- Transpulm. Gradient 24 mmHg
- Erhöhter RV-Füllungsdruck als Zeichen
der RV-Insuffizienz
Risikostratifizierung Frau A, 59-jährig

Alter > 70 Jahre (relativ) Symptomatische periphere oder cerebrale
Vaskulopathien Schwerer Diabetes mit Endorganschädigungen
(relativ) Schwere Lungenerkrankung (FVC und FEV1 < 40%) Erhöhtes Risiko „lebensbedrohender Noncompliance“
Aktiver Drogenabusus, schwere kognitive Störung, Umfeld
Aktive und/oder maligne Tumoren (< 5 Jahre tumorfrei) BMI >35 Chronische, schwer therapierbare Infekte Fixierte pulmonale Hypertonie > 4-5 Wood-Units,
PAPsyst. >60mmHg, TPG >15mmHg
HTx: Kontraindikationen I
0
10
20
30
40
50
60
2005 2006 2007 2008 2009 2010 2011 2012 2013 2014 2015 2016
% o
f P
ati
en
ts
Year of Transplant
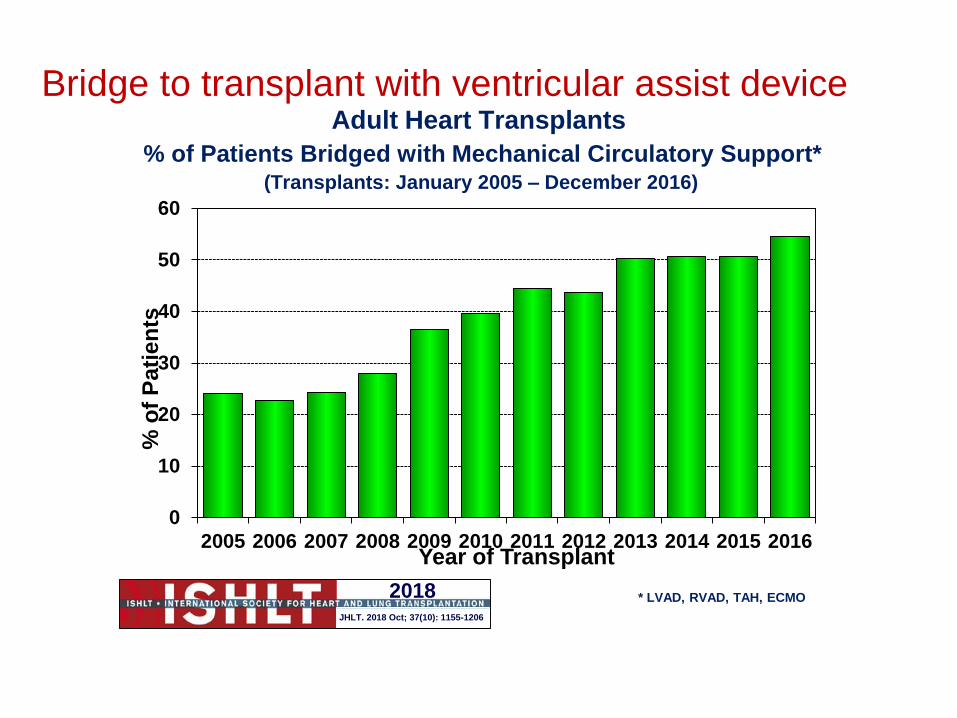
* LVAD, RVAD, TAH, ECMO
Adult Heart Transplants
% of Patients Bridged with Mechanical Circulatory Support*(Transplants: January 2005 – December 2016)
2018JHLT. 2018 Oct; 37(10): 1155-1206
Bridge to transplant with ventricular assist device
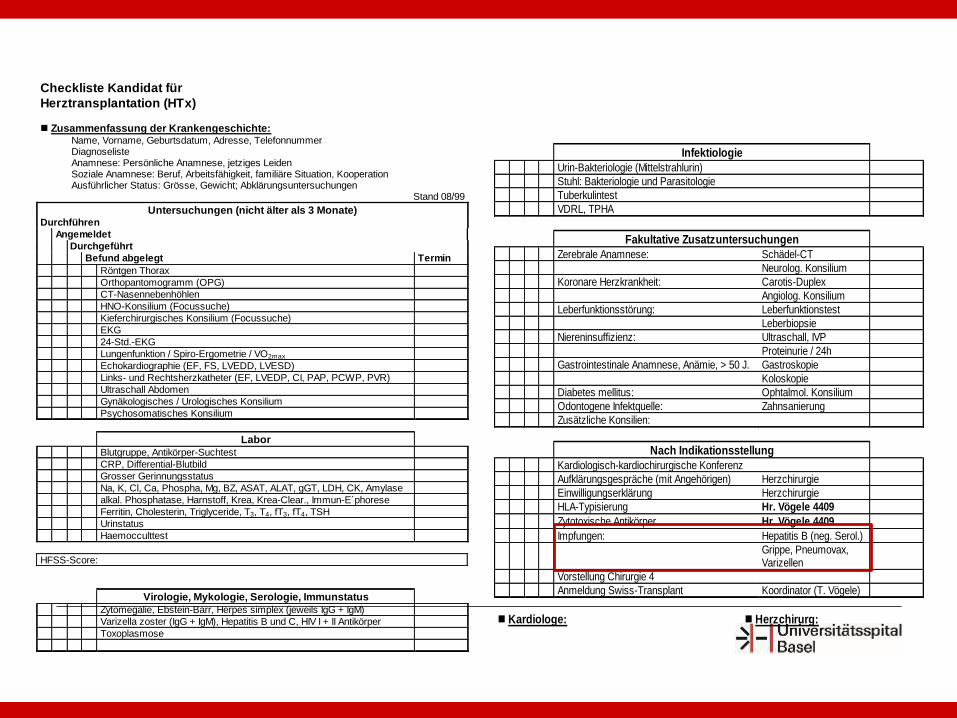
Checkliste Kandidat für
Herztransplantation (HTx)
Zusammenfassung der Krankengeschichte: Name, Vorname, Geburtsdatum, Adresse, Telefonnummer Diagnoseliste Anamnese: Persönliche Anamnese, jetziges Leiden Soziale Anamnese: Beruf, Arbeitsfähigkeit, familiäre Situation, Kooperation Ausführlicher Status: Grösse, Gewicht; Abklärungsuntersuchungen
Stand 08/99
Untersuchungen (nicht älter als 3 Monate) Durchführen
Angemeldet
Durchgeführt
Befund abgelegt Termin
Röntgen Thorax
Orthopantomogramm (OPG)
CT-Nasennebenhöhlen
HNO-Konsilium (Focussuche)
Kieferchirurgisches Konsilium (Focussuche)
EKG
24-Std.-EKG
Lungenfunktion / Spiro-Ergometrie / VO2max
Echokardiographie (EF, FS, LVEDD, LVESD)
Links- und Rechtsherzkatheter (EF, LVEDP, CI, PAP, PCWP, PVR)
Ultraschall Abdomen
Gynäkologisches / Urologisches Konsilium
Psychosomatisches Konsilium
Labor
Blutgruppe, Antikörper-Suchtest
CRP, Differential-Blutbild
Grosser Gerinnungsstatus
Na, K, Cl, Ca, Phospha, Mg, BZ, ASAT, ALAT, gGT, LDH, CK, Amylase
alkal. Phosphatase, Harnstoff, Krea, Krea-Clear., Immun-E´phorese
Ferritin, Cholesterin, Triglyceride, T3, T4, fT3, fT4, TSH
Urinstatus
Haemocculttest
HFSS-Score:
Virologie, Mykologie, Serologie, Immunstatus
Zytomegalie, Ebstein-Barr, Herpes simplex (jeweils IgG + IgM)
Varizella zoster (IgG + IgM), Hepatitis B und C, HIV I + II Antikörper
Toxoplasmose
Infektiologie
Urin-Bakteriologie (Mittelstrahlurin)
Stuhl: Bakteriologie und Parasitologie
Tuberkulintest
VDRL, TPHA
Fakultative Zusatzuntersuchungen
Zerebrale Anamnese: Schädel-CT
Neurolog. Konsilium
Koronare Herzkrankheit: Carotis-Duplex
Angiolog. Konsilium
Leberfunktionsstörung: Leberfunktionstest
Leberbiopsie
Niereninsuffizienz: Ultraschall, IVP
Proteinurie / 24h
Gastrointestinale Anamnese, Anämie, > 50 J. Gastroskopie
Koloskopie
Diabetes mellitus: Ophtalmol. Konsilium
Odontogene Infektquelle: Zahnsanierung
Zusätzliche Konsilien:
Nach Indikationsstellung
Kardiologisch-kardiochirurgische Konferenz
Aufklärungsgespräche (mit Angehörigen) Herzchirurgie
Einwilligungserklärung Herzchirurgie
HLA-Typisierung Hr. Vögele 4409
Zytotoxische Antikörper Hr. Vögele 4409
Impfungen: Hepatitis B (neg. Serol.)
Grippe, Pneumovax, Varizellen
Vorstellung Chirurgie 4
Anmeldung Swiss-Transplant Koordinator (T. Vögele)
Kardiologe: Herzchirurg:
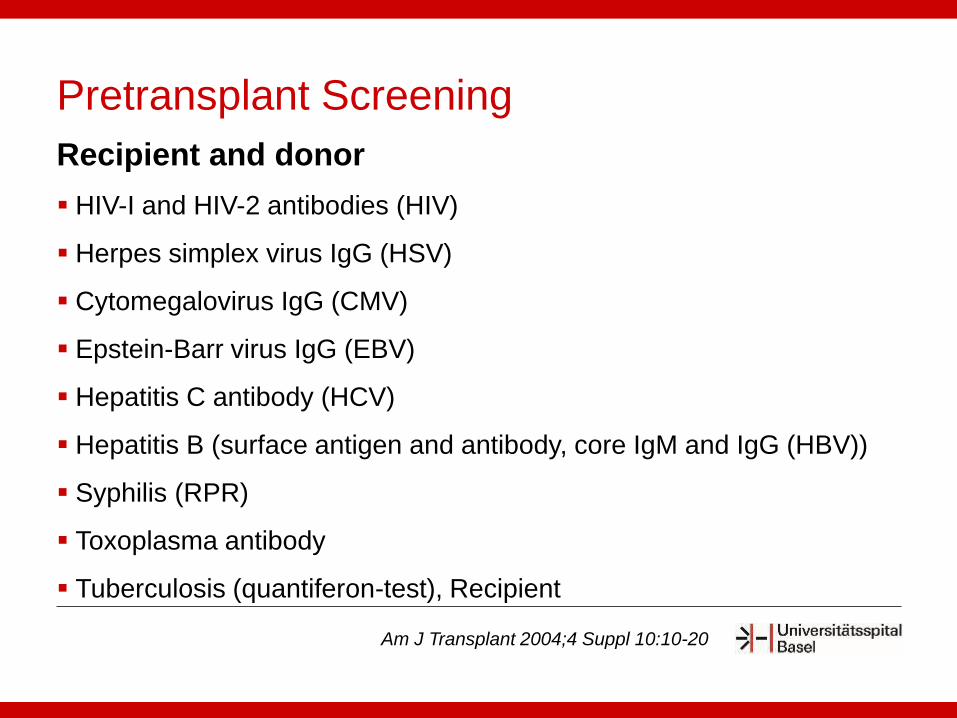
Pretransplant Screening
Recipient and donor
HIV-I and HIV-2 antibodies (HIV)
Herpes simplex virus IgG (HSV)
Cytomegalovirus IgG (CMV)
Epstein-Barr virus IgG (EBV)
Hepatitis C antibody (HCV)
Hepatitis B (surface antigen and antibody, core IgM and IgG (HBV))
Syphilis (RPR)
Toxoplasma antibody
Tuberculosis (quantiferon-test), Recipient
Am J Transplant 2004;4 Suppl 10:10-20


Standard Technik nach Lower and Shumway (biatrial)
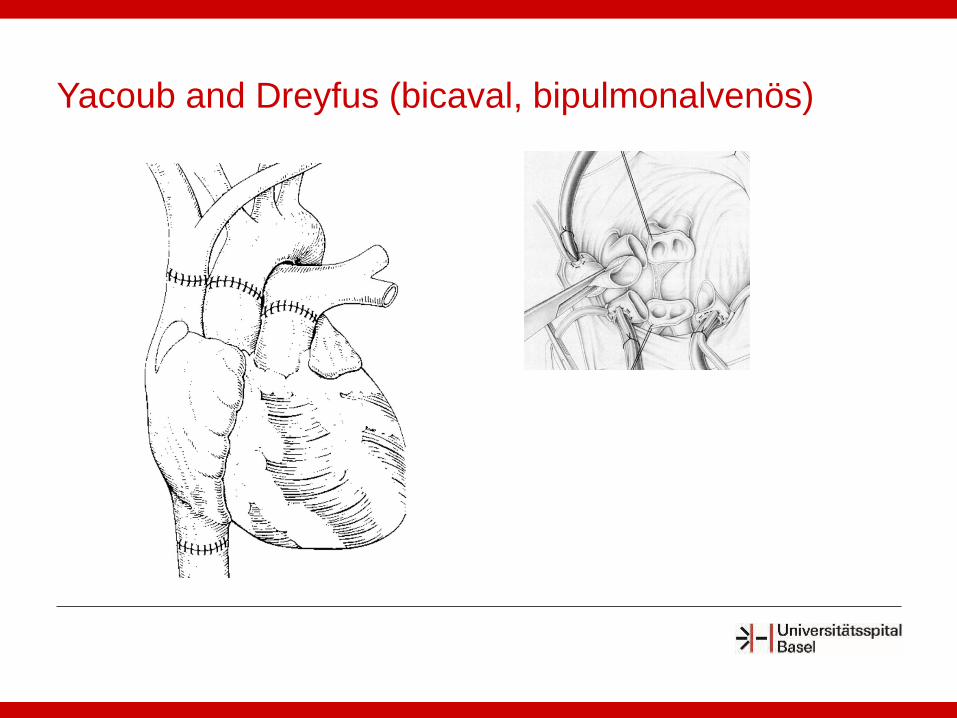
Yacoub and Dreyfus (bicaval, bipulmonalvenös)

Induktionstherapie
Erhaltungstherapie
Abstossungs-Therapie
Immunsuppression
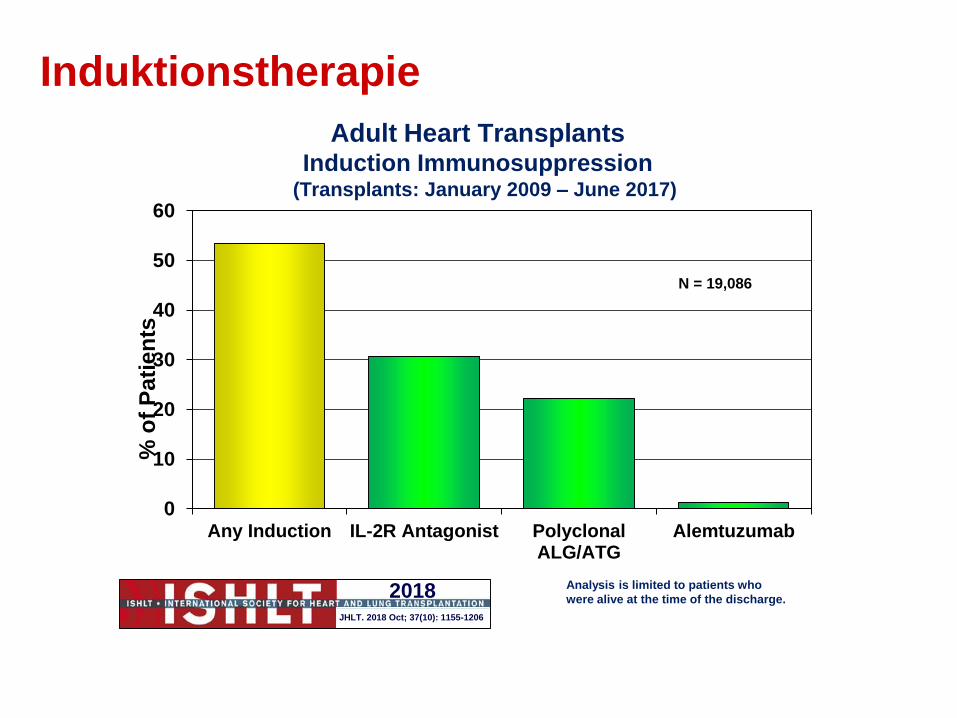
Analysis is limited to patients who
were alive at the time of the discharge.
0
10
20
30
40
50
60
Any Induction IL-2R Antagonist PolyclonalALG/ATG
Alemtuzumab
% o
f P
ati
en
tsAdult Heart Transplants
Induction Immunosuppression(Transplants: January 2009 – June 2017)
2018JHLT. 2018 Oct; 37(10): 1155-1206
N = 19,086
Induktionstherapie
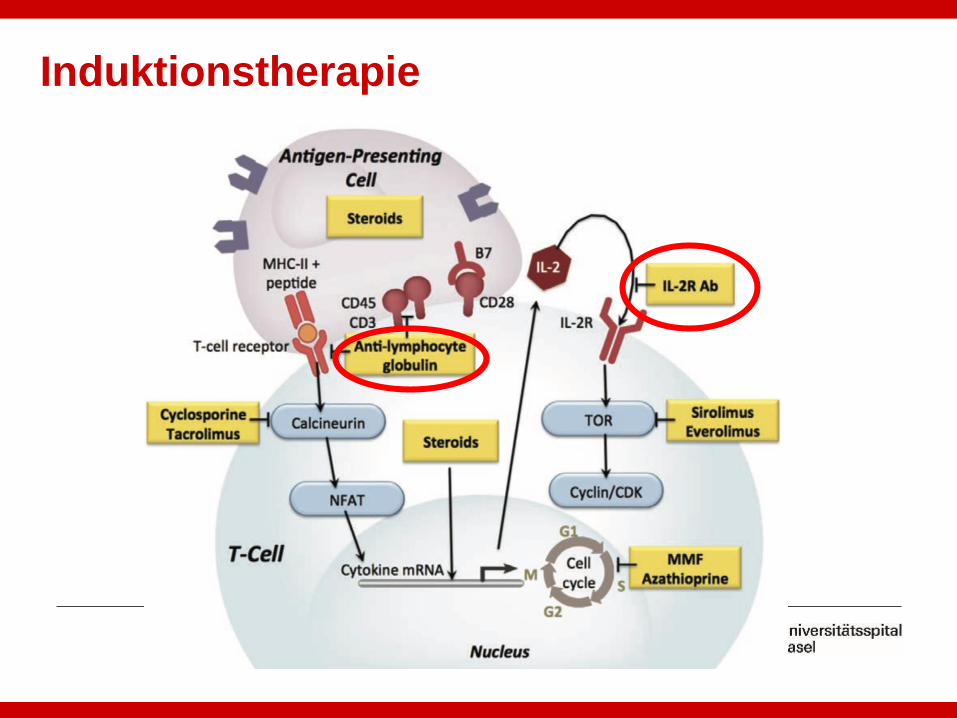
Induktionstherapie
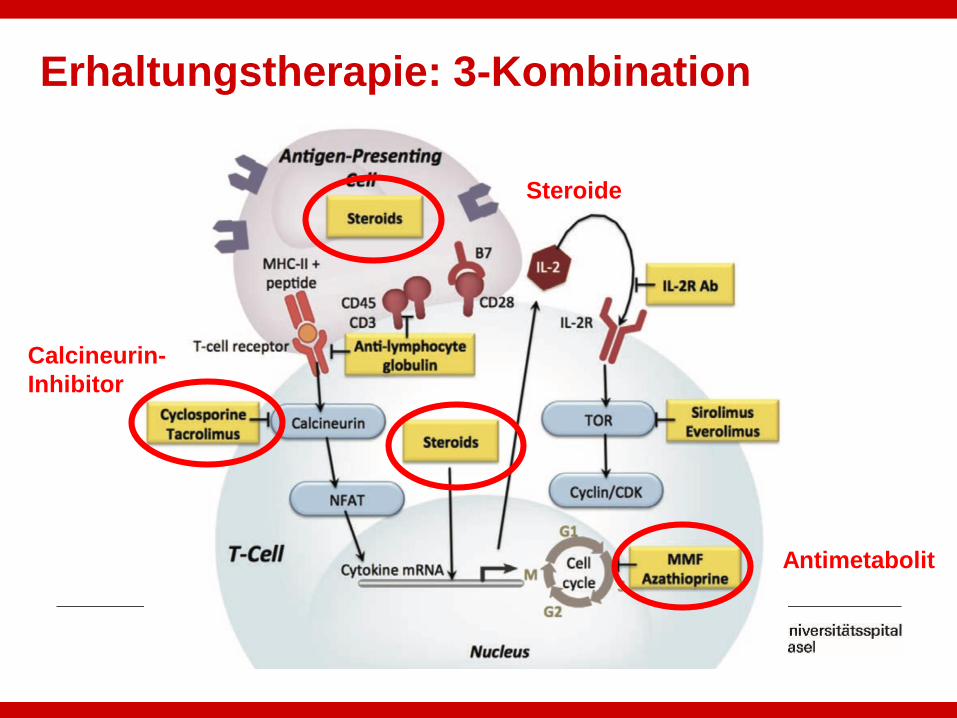
Erhaltungstherapie: 3-Kombination
Antimetabolit
Calcineurin-
Inhibitor
Steroide
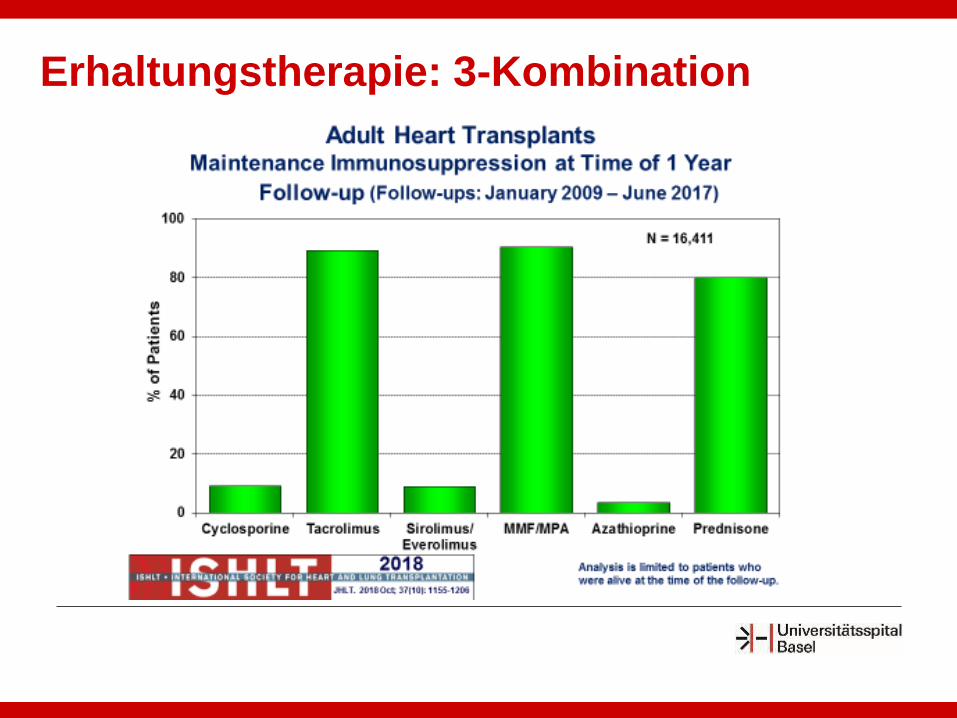
Erhaltungstherapie: 3-Kombination
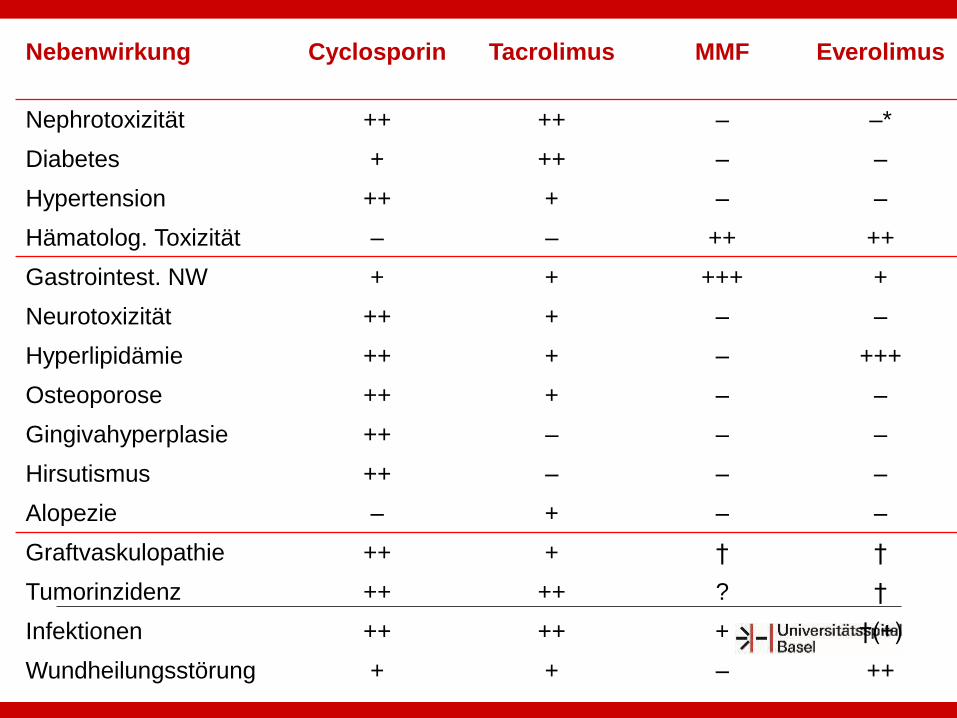
Nebenwirkung Cyclosporin Tacrolimus MMF Everolimus
Nephrotoxizität ++ ++ – –*
Diabetes + ++ – –
Hypertension ++ + – –
Hämatolog. Toxizität – – ++ ++
Gastrointest. NW + + +++ +
Neurotoxizität ++ + – –
Hyperlipidämie ++ + – +++
Osteoporose ++ + – –
Gingivahyperplasie ++ – – –
Hirsutismus ++ – – –
Alopezie – + – –
Graftvaskulopathie ++ + † †
Tumorinzidenz ++ ++ ? †
Infektionen ++ ++ + †(+)
Wundheilungsstörung + + – ++
• Kein klinisches Zeichen oder Symptom ist spezifisch für eine Abstossung
• Unspezifische körperliche Befunde
• Zeichen kardialer Irritation
• Zeichen/Symptome kardialer Dysfunktion und des „low cardiac output“ bei
schwerer Abstossung
• Aber: Die meisten Abstossungsepisoden sind asymptomatische
Zufallsbefunde (EMB)
Akute Abstossung: Klinische Manifestation
ISHLT 0: keine Abstossung
ISHLT 1R: leichte Abstossung (nicht therapiebedürftig)
ISHLT 2R: mittelschwere Abstossung (therapiebedürftig)
ISHLT 3R: schwere Abstossung (therapiebedürftig)
Akute zelluläre Abstossung(Klassifizierung n. ISHLT 2004)
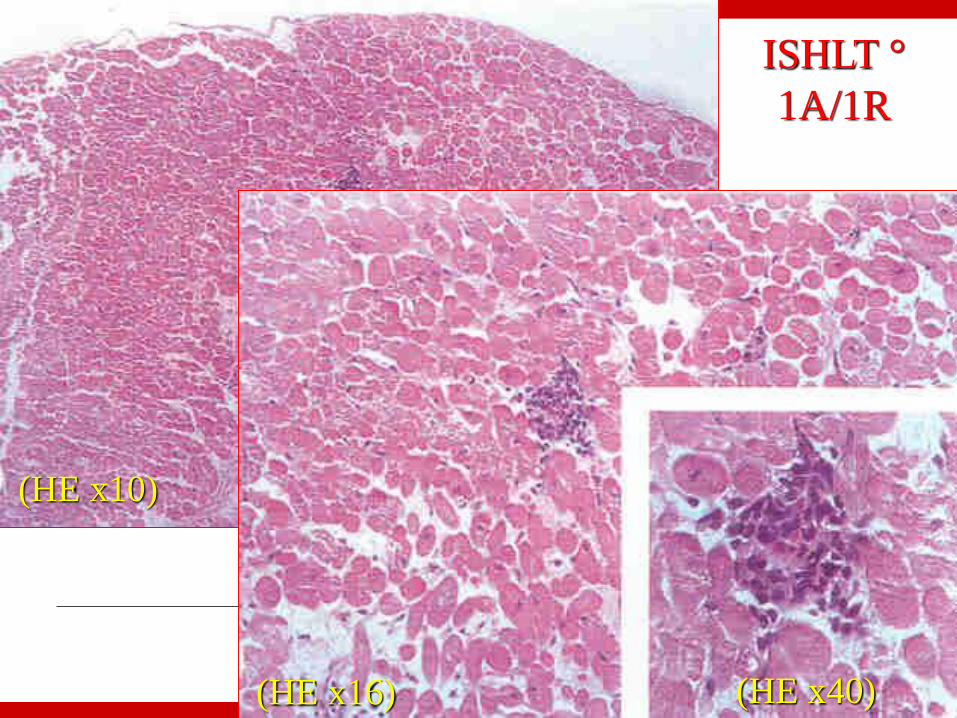
(HE x10)
ISHLT °
1A/1R
(HE x16) (HE x40)
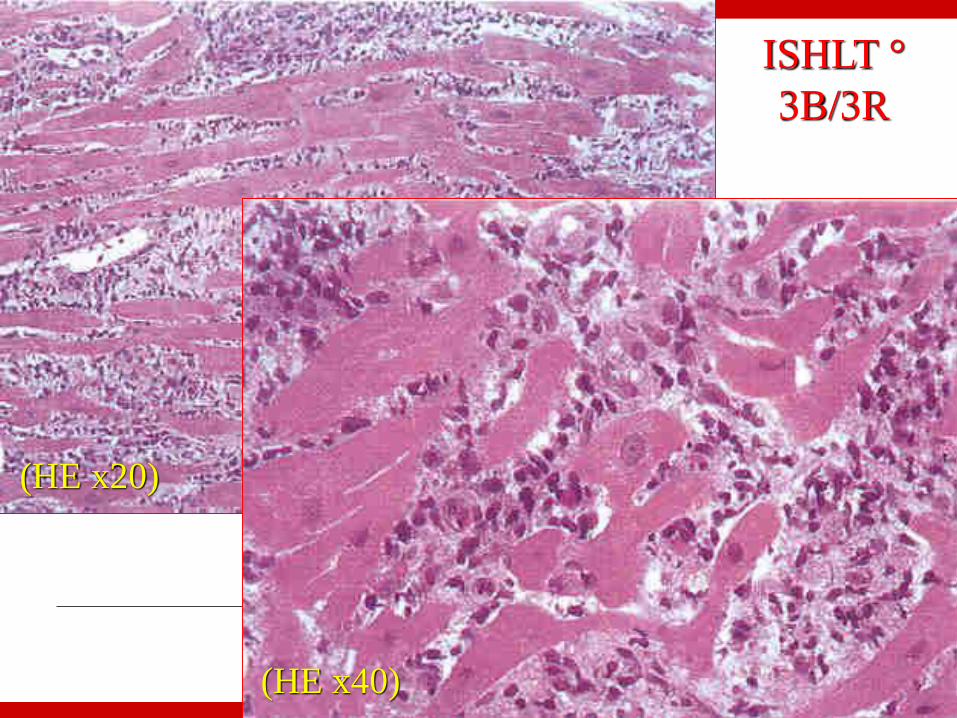
ISHLT °
3B/3R
(HE x20)
(HE x40)

ISHLT 2R: mittelschwere Abstossung (therapiebedürftig)
Prednison 3-5mg/kg pro Tag für 3-5 Tage
Solumedrol 0.5 – 1 g i.v. / pro Tag für 3 Tage
ISHLT 2 R mit hämodynamischer Kompromitierung;
oder ISHLT 3R (schwere Abstossung)
Antithymozyten Globulin (ATG)
OKT 3
Therapie der zellulären Abstossung
TT.MM.JJJJTitel/Anlass/Autor
38
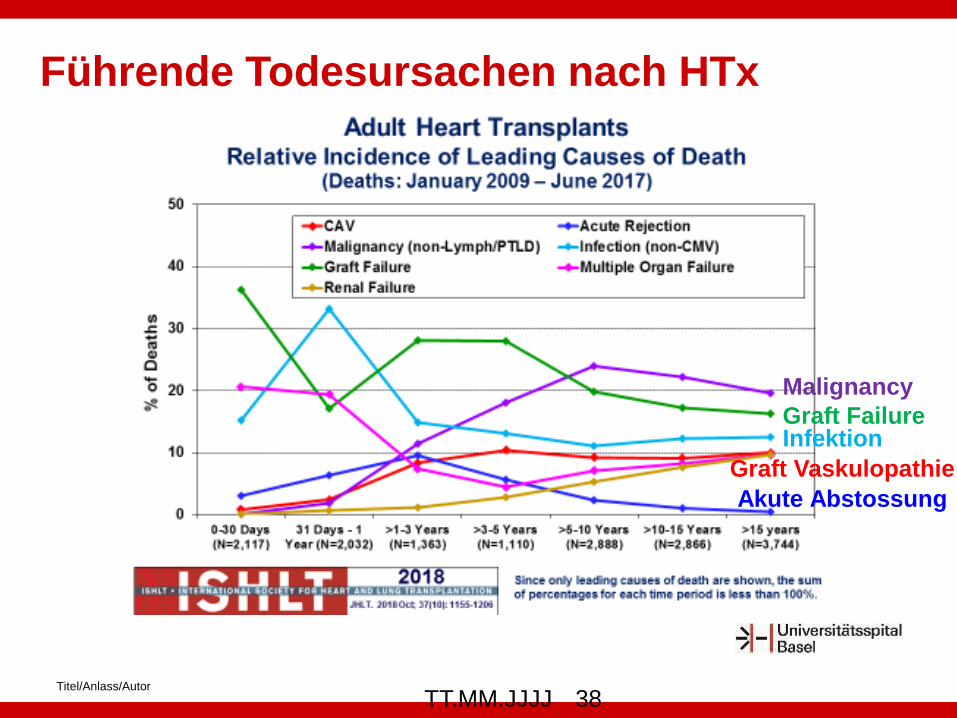
Malignancy
InfektionGraft Failure
Graft Vaskulopathie
Akute Abstossung
Führende Todesursachen nach HTx
Physiologie des transplantierten Herzens
Verminderter atrialer Kick und LV-Füllung bei biatrialer
Implantationstechnik; Verminderung des Schlagvolumens
Schnelle Ruheherzfrequenz (95 to 110 bpm) und träger
Herzfrequenzanstieg unter Belastung (denerviertes Herz)
Kein nächtliches Blutdruck-Dipping (denerviertes Herz)
Sehr häufig höhergradige diastolische Dysfunktion (niederschwellige
Abstossungsreaktion, Denervation, biatriale Anatomie)
Case: 52 year old male
April 30, 2017, heart transplantation
Hypertrophic cardiomyopathy
Bridge to transplant LVAD therapy 08/2015- 04/2017
May 15, 2017
Cytomegalovirus reactivation
Valgangciclovir 2x450mg
July 13, 2017
Presentation to the emergency department because of right sided
thoracic pain and fever (37.9°C). The pain was first recognized 7 days
ago.
Medication
Myfortic (Mycophenolate) Tbl 360 mg 360mg-0-360mg
Prograf (Tacrolimus) Kaps 5mg-0-4mg
Prednison Tabl. 25mg-0-0-0
Valcyte (Valganciclovir) Tabl 450mg-0-450mg
Bactrim forte Tabl 800/160 mg 1/2-0-0-0 (Mo/We/Fri)
Ampho-Moronal Susp 10% (24 ml) 1-1-1-1
Atorvastatin Tabl 40 20mg-0-0-0
Esomeprazol Tabl 40 mg 1-0-1-0
Calcimagon D3 1000 1-0-0-0
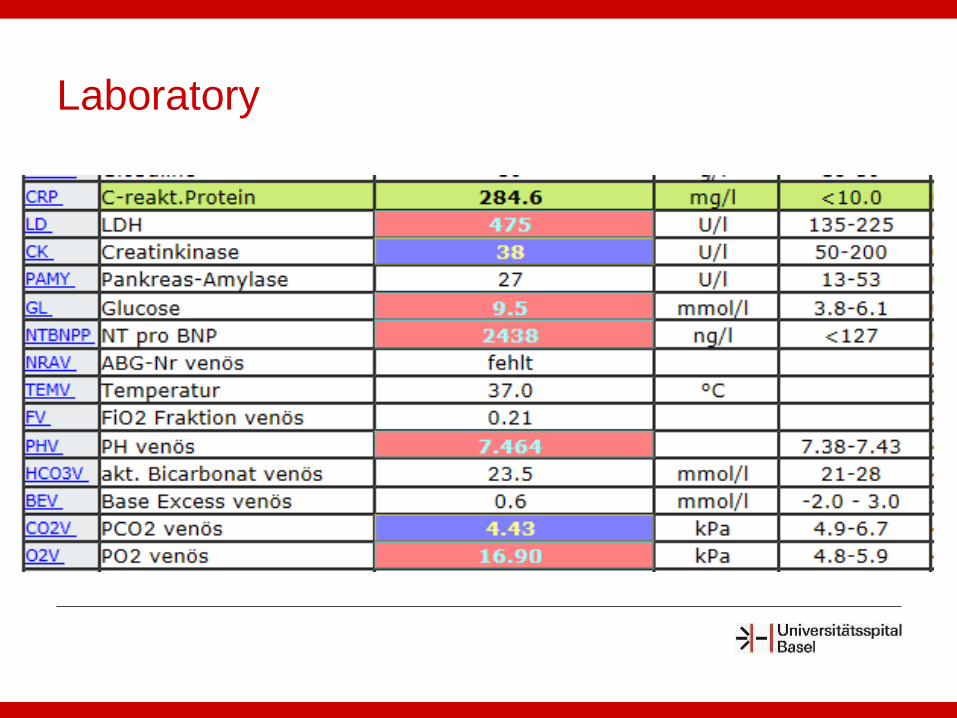
Laboratory
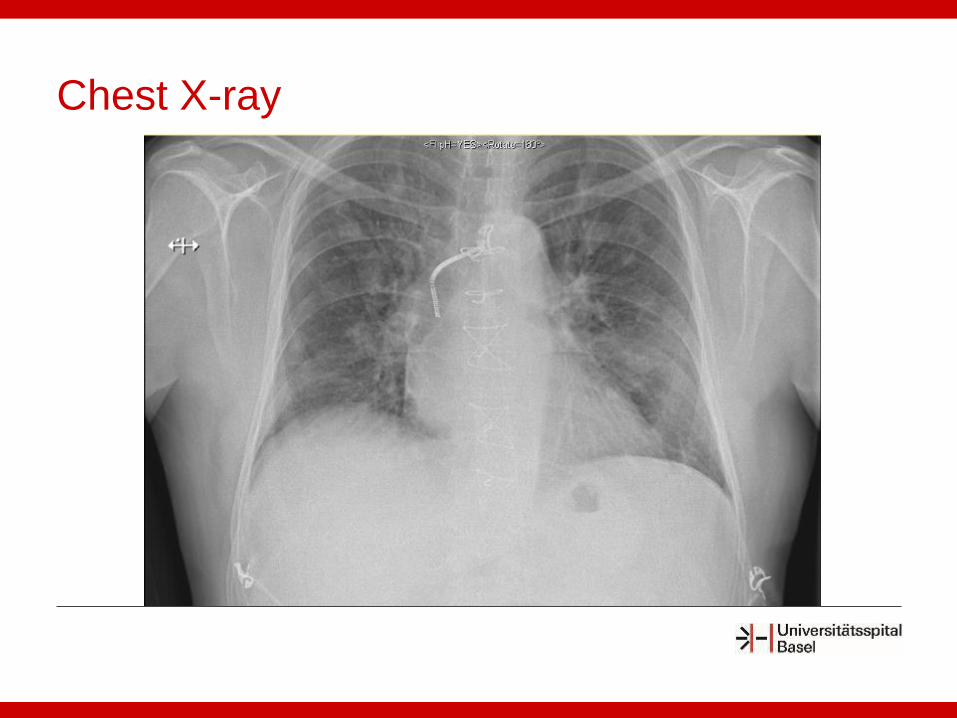
Chest X-ray

Chest CT
Fungal Pathogens
Most common: Candida, Aspergillus, Cryptococcus, Pneumocystis
intermediate and late posttransplant period
Candida
most common early (first month), catheter-related
Aspergillus
most common within the first year after transplant
significant morbidity and mortality
Presentation: invasive pulmonary disease, aspergilloma, rhinosinusitis
Risk factors: CMV disease, intensive immunosuppression, rejection,
renal dysfunction, environmental exposure (gardening)
Minari A et al. Transpl Infect Dis 2002
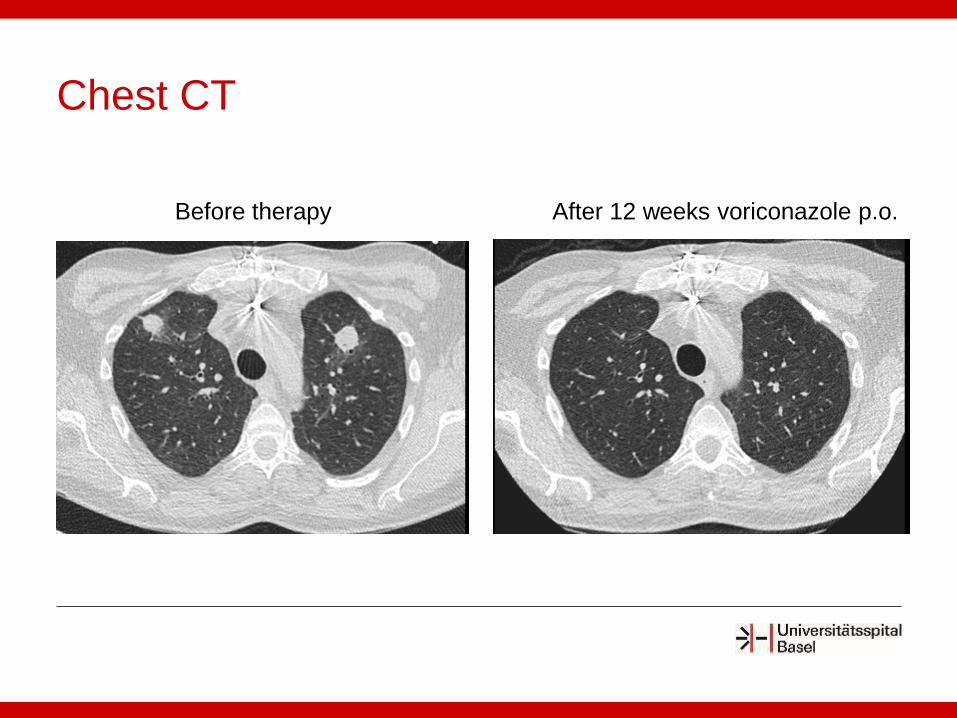
Chest CT
Before therapy After 12 weeks voriconazole p.o.
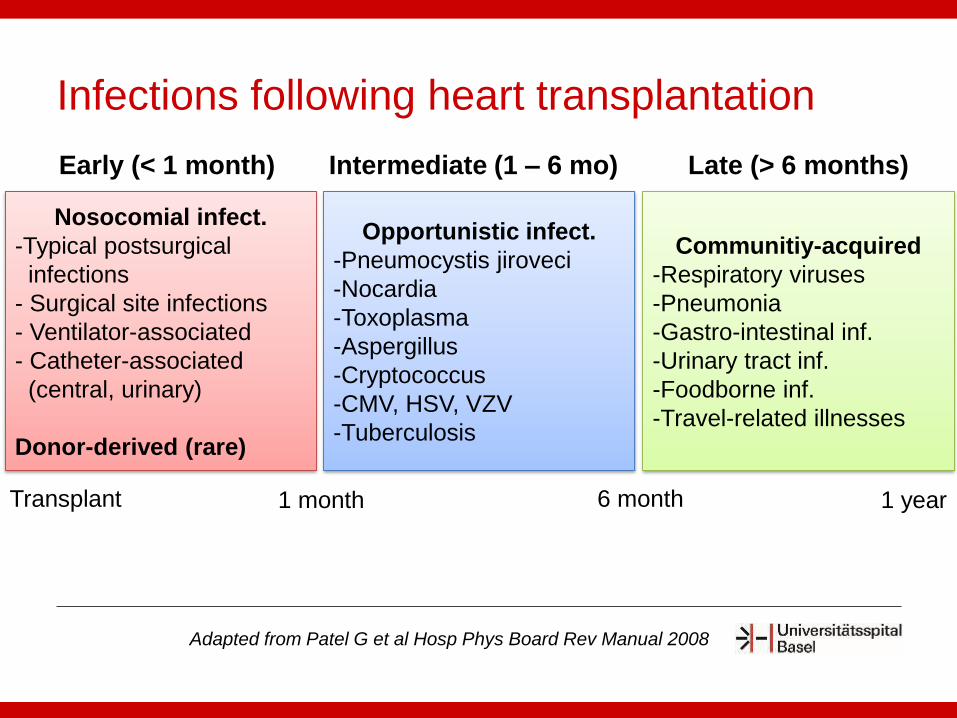
Infections following heart transplantation
Nosocomial infect.
-Typical postsurgical
infections
- Surgical site infections
- Ventilator-associated
- Catheter-associated
(central, urinary)
Donor-derived (rare)
Opportunistic infect.
-Pneumocystis jiroveci
-Nocardia
-Toxoplasma
-Aspergillus
-Cryptococcus
-CMV, HSV, VZV
-Tuberculosis
Communitiy-acquired
-Respiratory viruses
-Pneumonia
-Gastro-intestinal inf.
-Urinary tract inf.
-Foodborne inf.
-Travel-related illnesses
Early (< 1 month) Intermediate (1 – 6 mo) Late (> 6 months)
Transplant 1 month 6 month 1 year
Adapted from Patel G et al Hosp Phys Board Rev Manual 2008
TT.MM.JJJJTitel/Anlass/Autor
48
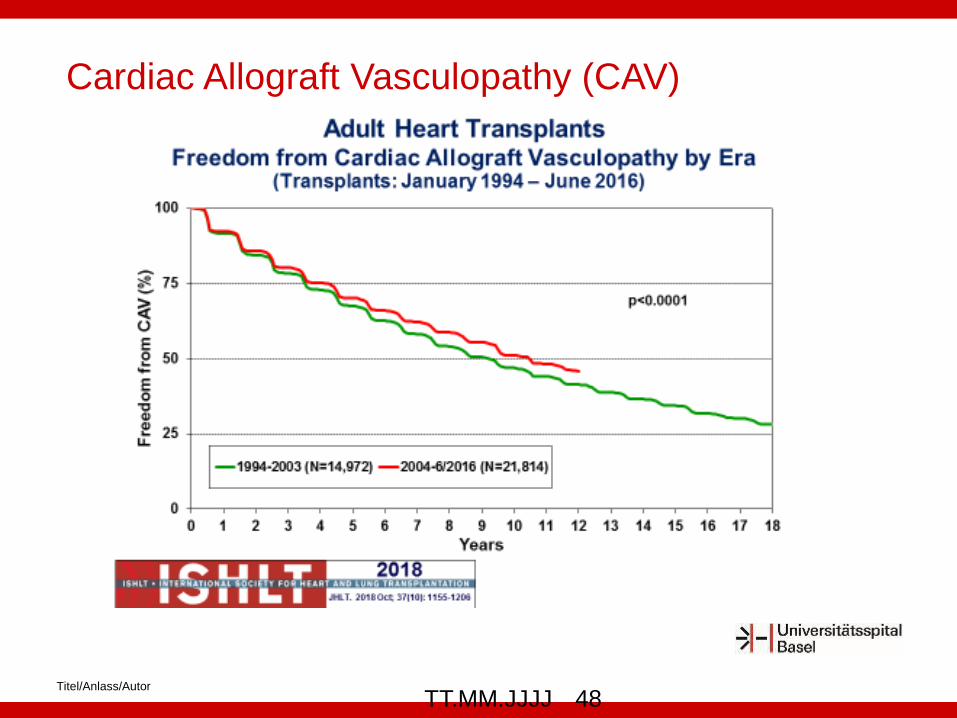
Cardiac Allograft Vasculopathy (CAV)
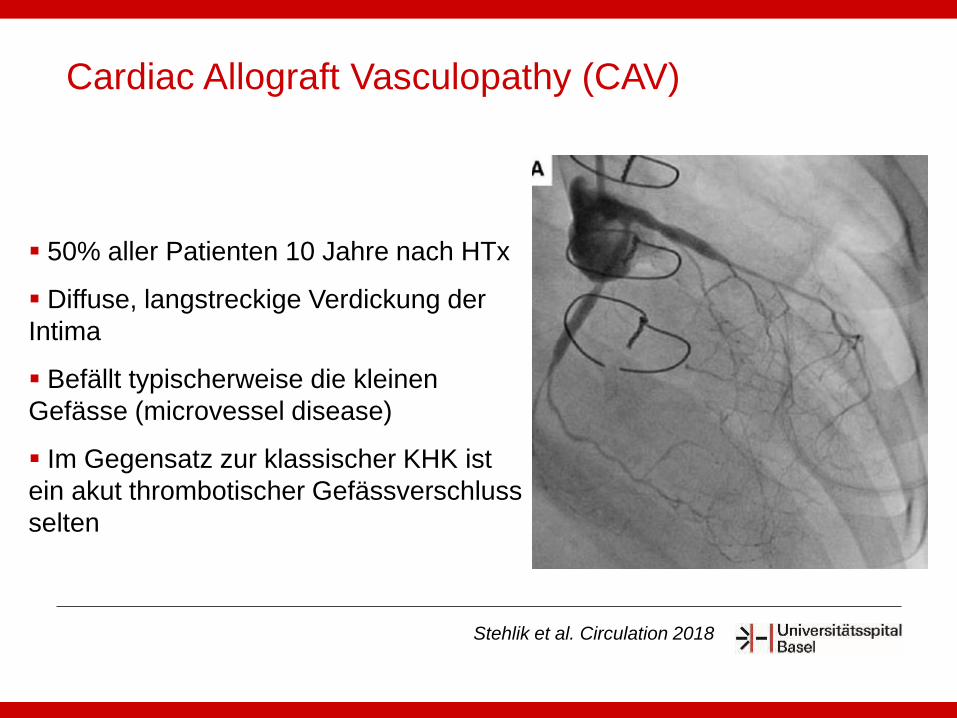
50% aller Patienten 10 Jahre nach HTx
Diffuse, langstreckige Verdickung der
Intima
Befällt typischerweise die kleinen
Gefässe (microvessel disease)
Im Gegensatz zur klassischer KHK ist
ein akut thrombotischer Gefässverschluss
selten
Cardiac Allograft Vasculopathy (CAV)
Stehlik et al. Circulation 2018
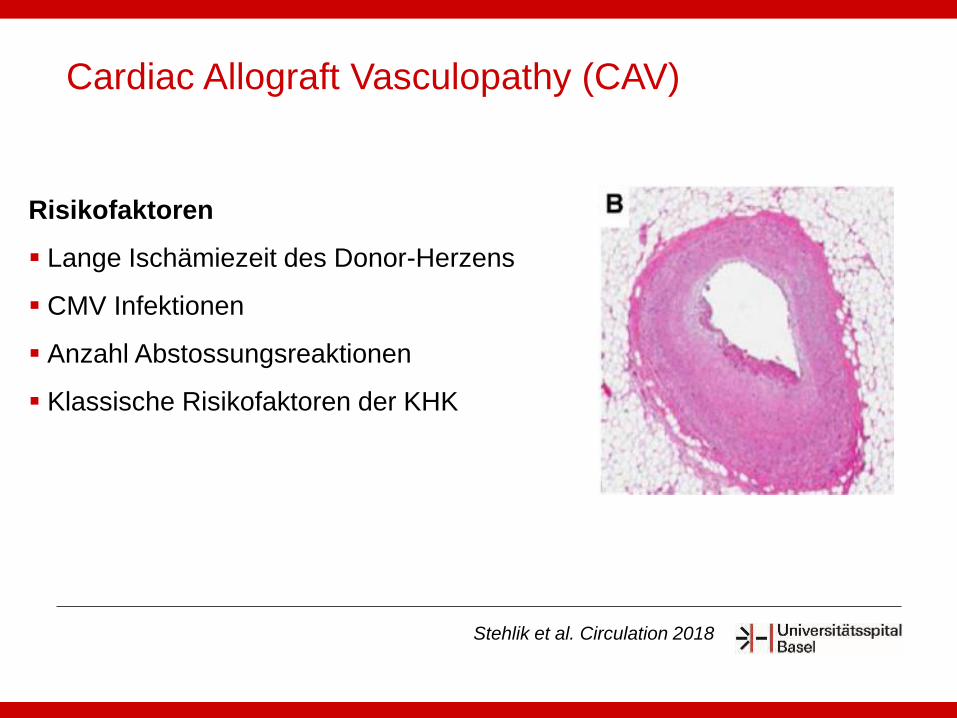
Risikofaktoren
Lange Ischämiezeit des Donor-Herzens
CMV Infektionen
Anzahl Abstossungsreaktionen
Klassische Risikofaktoren der KHK
Cardiac Allograft Vasculopathy (CAV)
Stehlik et al. Circulation 2018
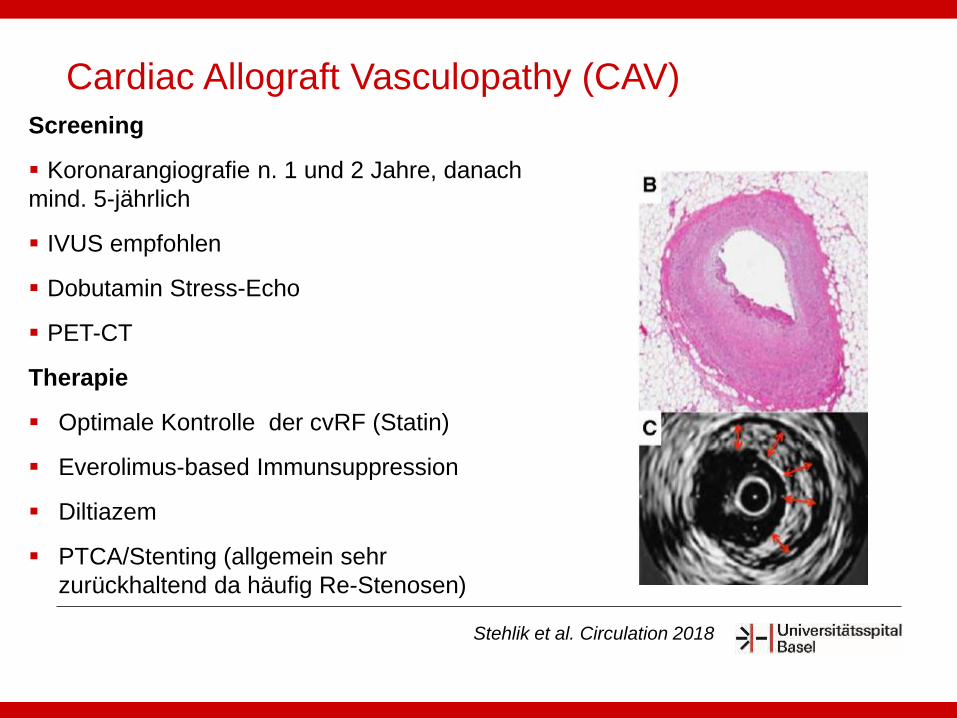
Screening
Koronarangiografie n. 1 und 2 Jahre, danach
mind. 5-jährlich
IVUS empfohlen
Dobutamin Stress-Echo
PET-CT
Therapie
Optimale Kontrolle der cvRF (Statin)
Everolimus-based Immunsuppression
Diltiazem
PTCA/Stenting (allgemein sehr
zurückhaltend da häufig Re-Stenosen)
Cardiac Allograft Vasculopathy (CAV)
Stehlik et al. Circulation 2018
Titel/Anlass/Autor
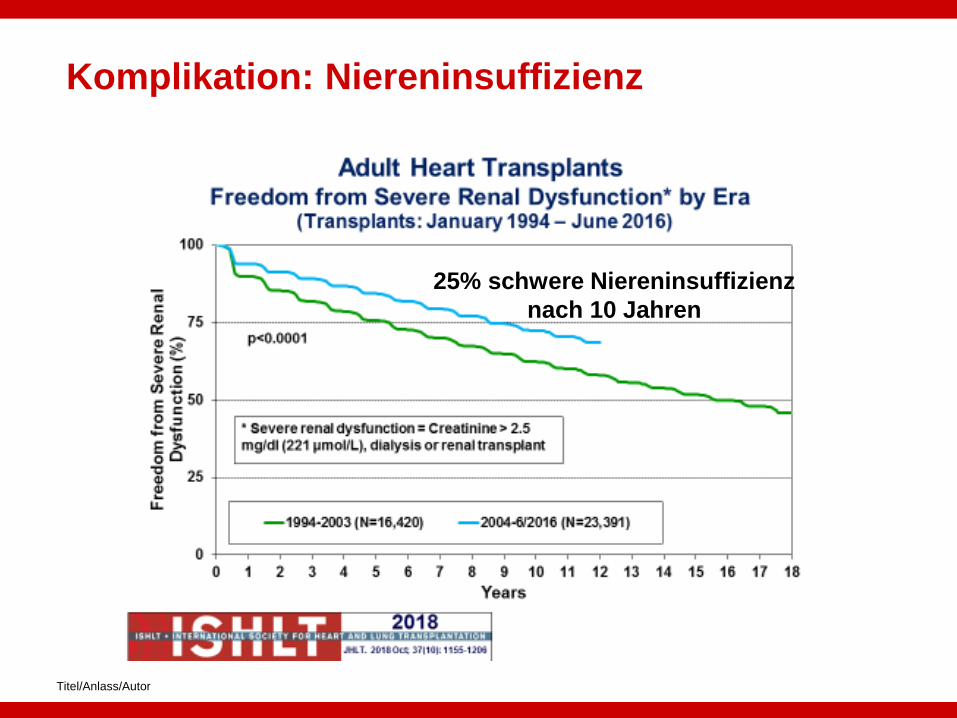
Komplikation: Niereninsuffizienz
25% schwere Niereninsuffizienz
nach 10 Jahren
Titel/Anlass/Autor
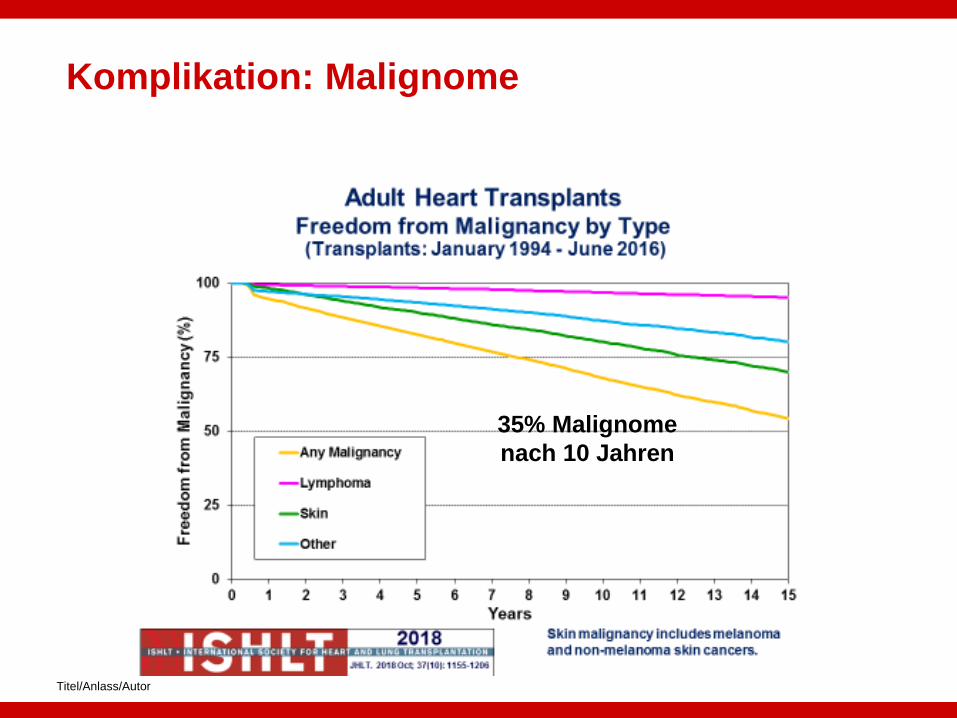
Komplikation: Malignome
35% Malignome
nach 10 Jahren
Überwachen der Immunsuppression (Medikamentenspiegel); 3-
6 monatlich
Kontrolle/Behandlung der NW der Immunsuppression
Arterielle Hypertonie, Dyslipidämie, Niereninsuffizienz,
Diabetes, Osteoporose, Infektionen, Neuropathie
Überwachung der Herzfunktion / Abstossung / Transplantat-
Vaskulopathie
Echo (6-12 monatlich) / Stressecho, Herzbiopsie,
Koronarangiografie
Screening für Neoplasien
Tranplantationsnachsorge

Bei einem jährlichen Mortalitätsrisiko von > 20% sollte eine
Herzersatztherapie evaluiert werden (HTx / VAD)
Das mediane Überleben nach HTx ist in den letzten 30 Jahren
kontinuierlich gestiegen (aktuell 12.5 Jahre)
Herzbiopsien sind in den ersten 2 Jahren zentral. Langfristige,
jährliche Protokollbiopsien haben an Bedeutung verloren
Die kardiale Allograft Vaskulopathie (CAV) ist sehr häufig (50%
n. 10 Jahren), bestimmt die langfristige Prognose und stellt eine
therapeutische Herausforderung dar
Die Langzeit-Prognose ist entscheidend durch die CAV und die
Nebenwirkungen der Immunsuppression geprägt
Calcineurin-Inhibitoren (Sandimmun, Tacrolimus) und mTOR-
Inhibitoren (Everolimus) haben ausgeprägte Medikamenten-
Wechselwirkungen
Take home messages

www.cardiobasel.ch
Vielen Dank

Immunsuppressiva: Wirkungsmechanismus
Direct effects
– Asymptomatic viral shedding
– Acute viral syndrome, flu like symptoms (fever,
malaise, headaches, diarrhea)
– Tissue invasive disease: colitis, esophagitis, oral
ulcers, pneumonitis, hepatitis, nephritis, retinitis
– Infection of allograft: myocarditis
Clinical manifestations of CMV infection
Patel G et al Hosp Phys Board Rev Manual 2008
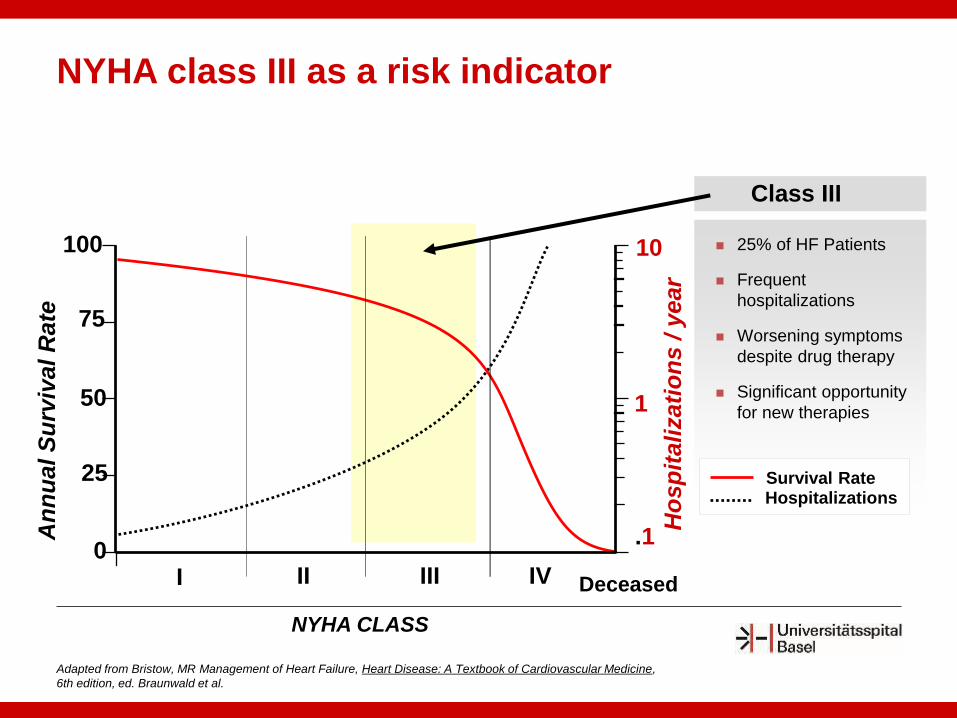
100
75
50
25
0I II III IV
1
10
NYHA CLASS
An
nu
al S
urv
ival
Rate
Ho
sp
itali
zati
on
s / y
ear
.1
Deceased
Adapted from Bristow, MR Management of Heart Failure, Heart Disease: A Textbook of Cardiovascular Medicine,
6th edition, ed. Braunwald et al.
Class III
25% of HF Patients
Frequent
hospitalizations
Worsening symptoms
despite drug therapy
Significant opportunity
for new therapies
Survival RateHospitalizations
NYHA class III as a risk indicator
Recurrent heart failure hospitalisations
Recurrent ventricular tachycardia, electrical storm
Development of cardiorenal syndrome
Intolerability of RAAS inhibiting drugs
Hyponatremia
Poor right heart function
High NT-proBNP > 5000
Red flags for a bad prognosis
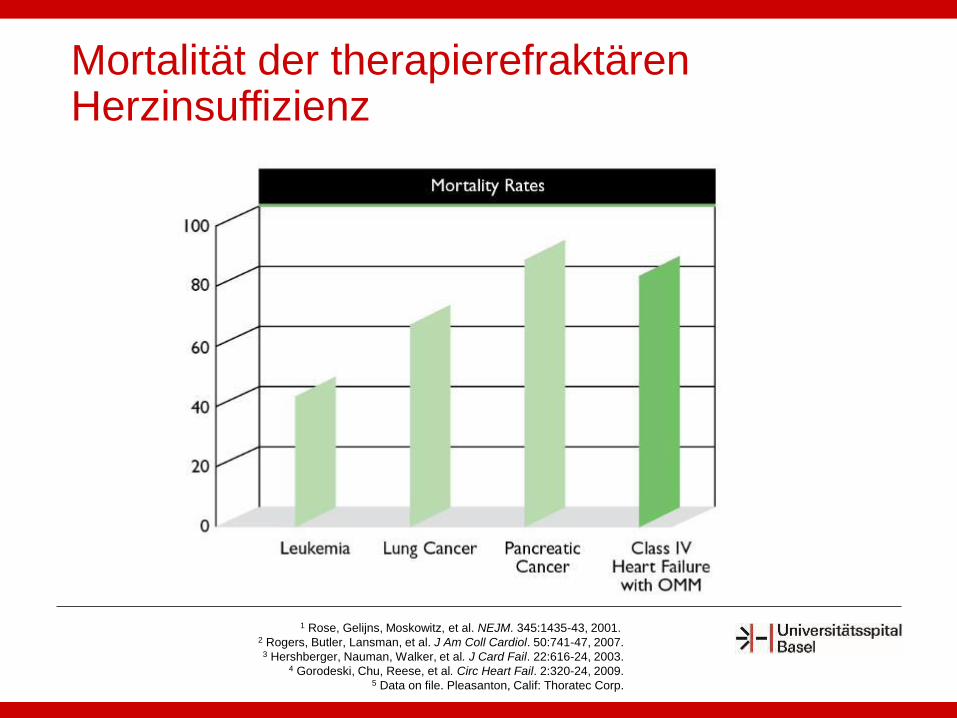
1 Rose, Gelijns, Moskowitz, et al. NEJM. 345:1435-43, 2001. 2 Rogers, Butler, Lansman, et al. J Am Coll Cardiol. 50:741-47, 2007.
3 Hershberger, Nauman, Walker, et al. J Card Fail. 22:616-24, 2003.4 Gorodeski, Chu, Reese, et al. Circ Heart Fail. 2:320-24, 2009.
5 Data on file. Pleasanton, Calif: Thoratec Corp.
Mortalität der therapierefraktären Herzinsuffizienz
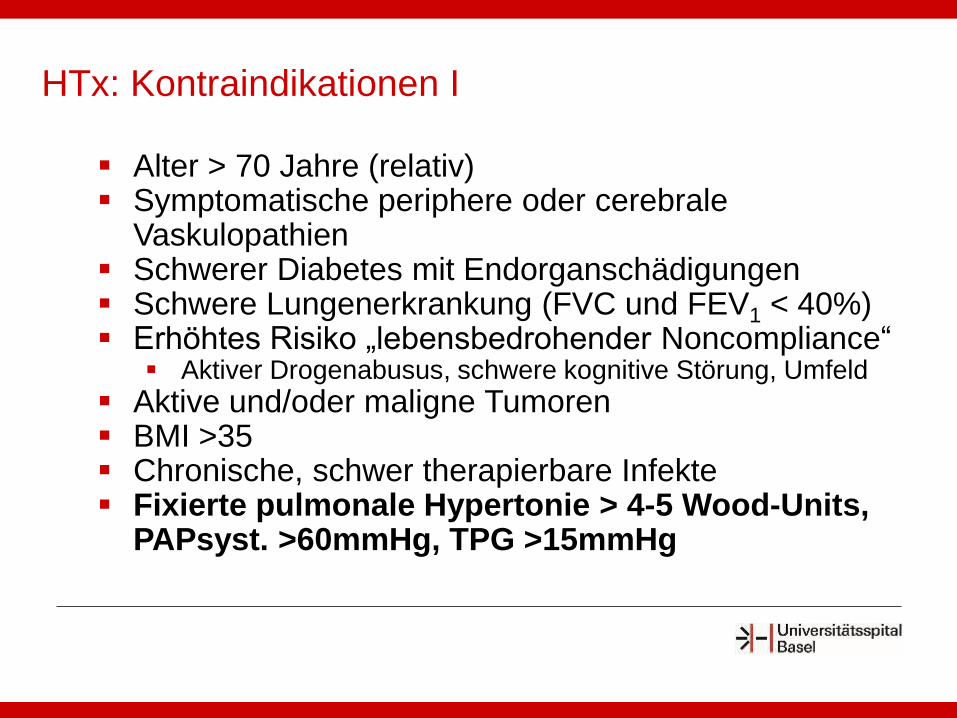
Alter > 70 Jahre (relativ) Symptomatische periphere oder cerebrale
Vaskulopathien Schwerer Diabetes mit Endorganschädigungen Schwere Lungenerkrankung (FVC und FEV1 < 40%) Erhöhtes Risiko „lebensbedrohender Noncompliance“
Aktiver Drogenabusus, schwere kognitive Störung, Umfeld
Aktive und/oder maligne Tumoren BMI >35 Chronische, schwer therapierbare Infekte Fixierte pulmonale Hypertonie > 4-5 Wood-Units,
PAPsyst. >60mmHg, TPG >15mmHg
HTx: Kontraindikationen I
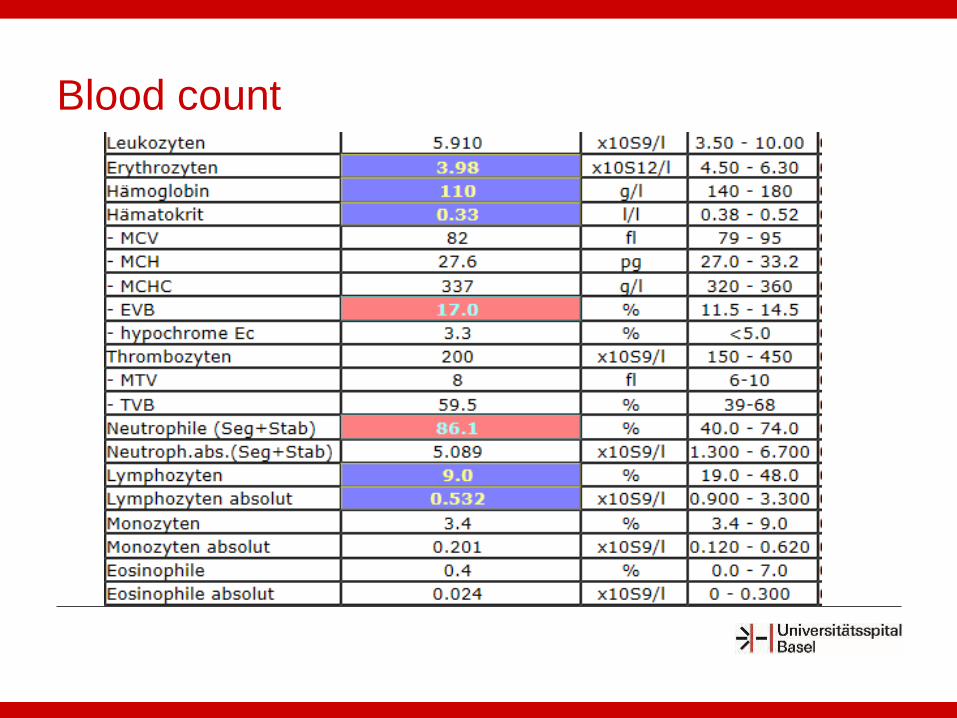
Blood count
Treatment of Aspergillosis
Voriconazole (first-line therapy)
significant interaction with calcineurin and TOR inhibitors
reduction and close monitoring of calcineurin and TOR inhibitors
Amphotericin B (second-line therapy)
renal toxicity
Surgery (resection of aspergilloma)
Should be considered and persued when feasible
Walsh TJ et al. Clin Infect Dis 2008
Posttransplant Prophylaxis
Trimethoprim-sulfamethoxazole (TMP-SMX): (3 times a week)
Pneumocystis pneumonia
Toxoplasmosis
Listeria monocytogenes
Valganciclovir
Cytomegalovirus

Direct effects
– Flu like symptoms (fever,
malaise, headaches,
diarrhea)
– Tissue invasive disease:
colitis, esophagitis, oral
ulcers, pneumonitis,
hepatitis, nephritis,
retinitis
– Myocarditis
Clinical manifestations of CMV infection
Patel G et al Hosp Phys Board Rev Manual 2008
Indirect effects
– Allograft rejection
– Graft vasculopathy
– Promotion of other
infections (bacterial,
fungal)

Major viral pathogen in solid organ
transplantation
Serologic status: most important risk factor
Highest risk: donor+/ recepient- (D+/R-)
Reactivation of latent CMV infection in
recepient+ (D-/R+)
Cytomegalovirus (CMV)
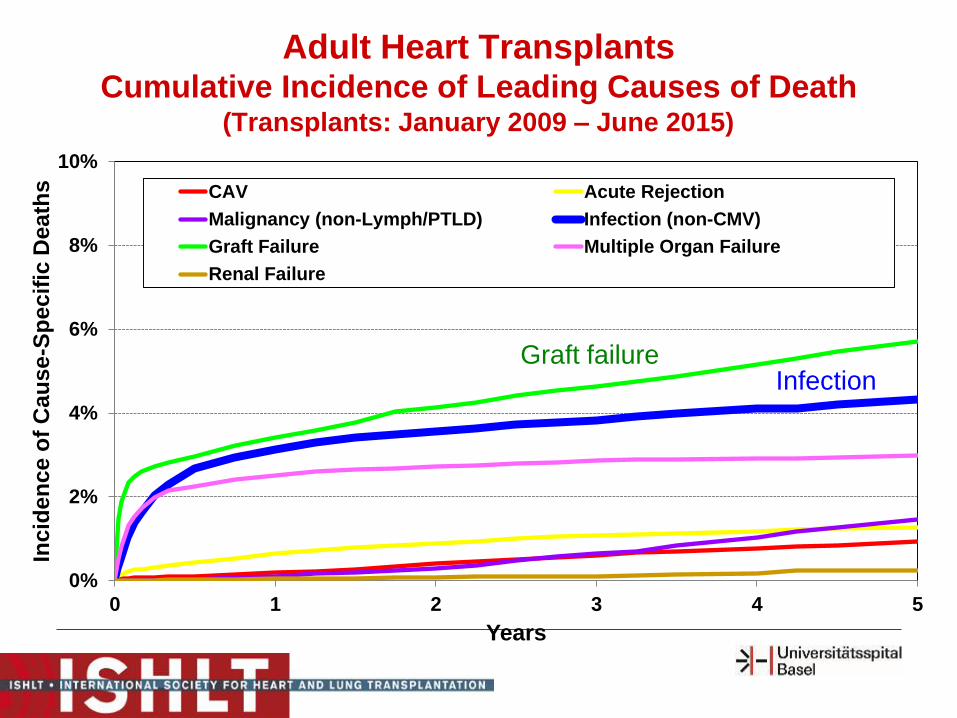
0%
2%
4%
6%
8%
10%
0 1 2 3 4 5
Inc
ide
nc
e o
f C
au
se
-Sp
ec
ific
De
ath
s
Years
CAV Acute Rejection
Malignancy (non-Lymph/PTLD) Infection (non-CMV)
Graft Failure Multiple Organ Failure
Renal Failure
2017JHLT. 2017 Oct; 36(10): 1037-1079
Adult Heart TransplantsCumulative Incidence of Leading Causes of Death
(Transplants: January 2009 – June 2015)
InfectionGraft failure
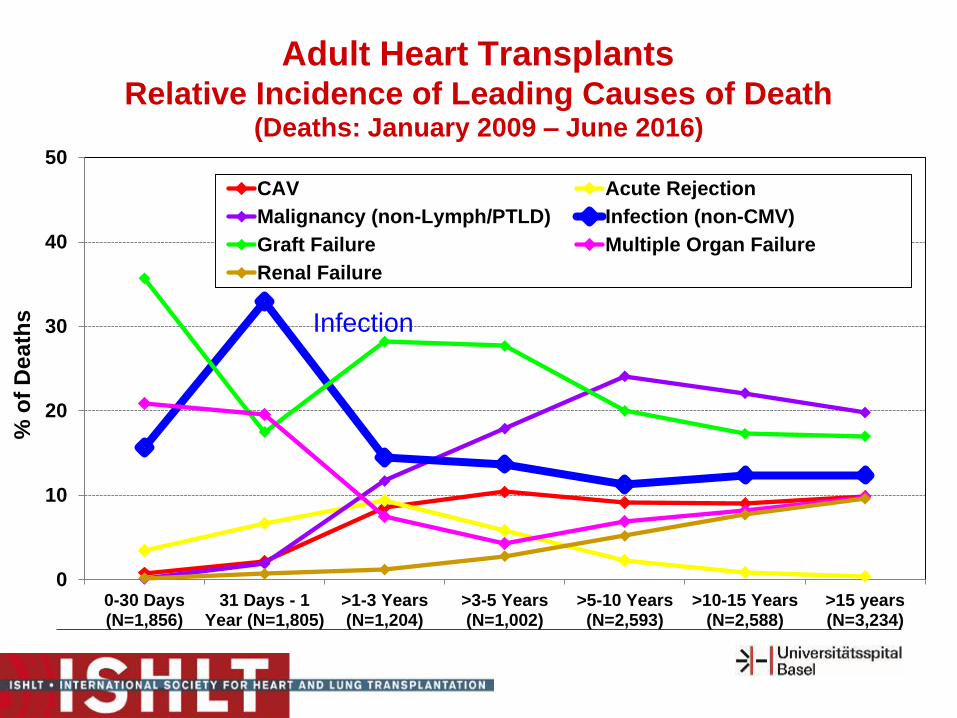
0
10
20
30
40
50
0-30 Days(N=1,856)
31 Days - 1Year (N=1,805)
>1-3 Years(N=1,204)
>3-5 Years(N=1,002)
>5-10 Years(N=2,593)
>10-15 Years(N=2,588)
>15 years(N=3,234)
% o
f D
ea
ths
CAV Acute Rejection
Malignancy (non-Lymph/PTLD) Infection (non-CMV)
Graft Failure Multiple Organ Failure
Renal Failure
2017JHLT. 2017 Oct; 36(10): 1037-1079
Adult Heart Transplants Relative Incidence of Leading Causes of Death
(Deaths: January 2009 – June 2016)
Infection
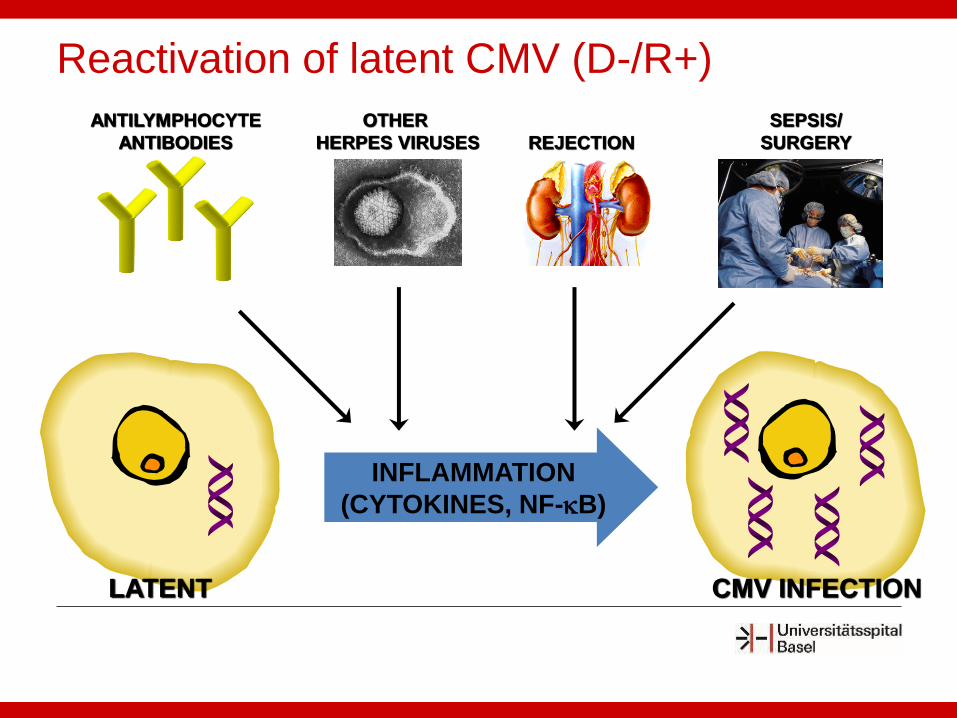
INFLAMMATION
(CYTOKINES, NF-B)
LATENT
ANTILYMPHOCYTE
ANTIBODIES
OTHER
HERPES VIRUSES
SEPSIS/
SURGERYREJECTION
CMV INFECTION
Reactivation of latent CMV (D-/R+)
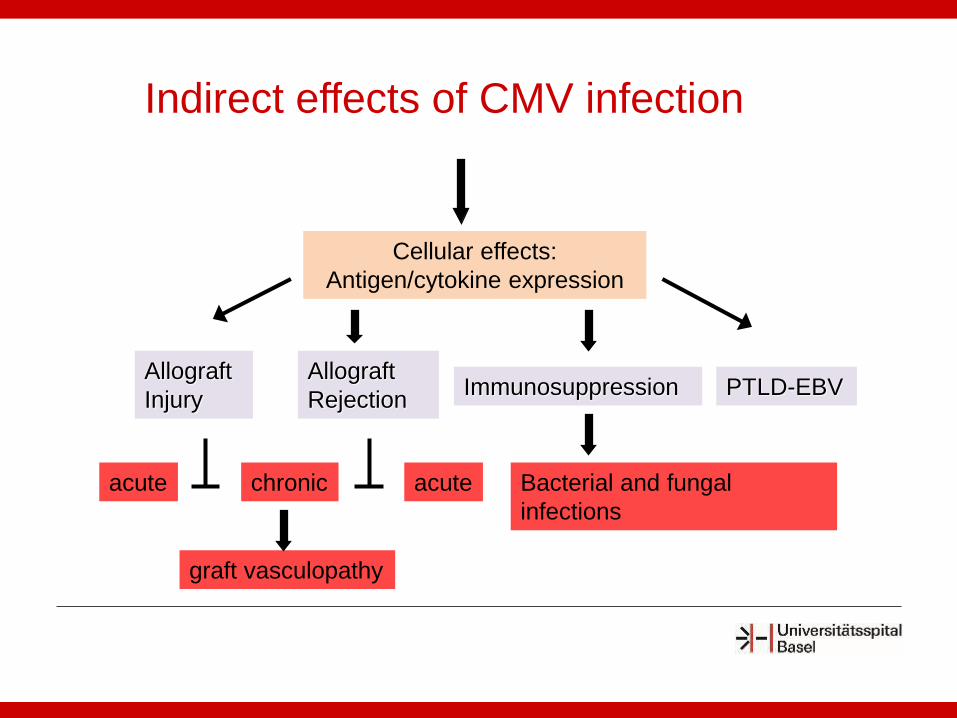
Cellular effects:
Antigen/cytokine expression
PTLD-EBVImmunosuppression
Bacterial and fungal
infections
Allograft
Injury
Allograft
Rejection
graft vasculopathy
chronicacute acute
Indirect effects of CMV infection

















