

Personalisierte Medizin in der PraxisDr. Bernhard KirschbaumDVFA Life Science ConferenceFrankfurt, 17. Juni 2009
2
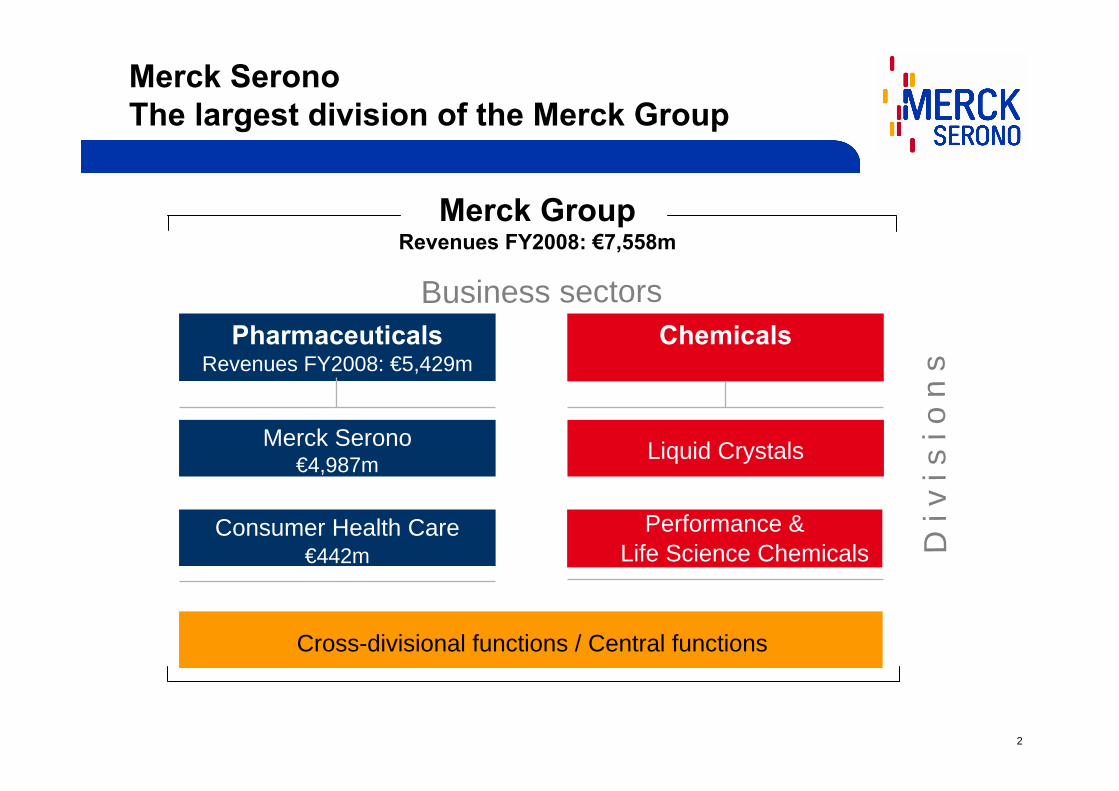
Merck SeronoThe largest division of the Merck Group
PharmaceuticalsRevenues FY2008: €5,429m
Merck Serono€4,987m
Chemicals
Consumer Health Care€442m
Liquid Crystals
Cross-divisional functions / Central functions
Merck GroupRevenues FY2008: €7,558m
D i
v i s
i o
n s
Business sectors
Performance & Life Science Chemicals

3
Merck Serono –Key Facts & Figures
Established: January 5, 2007
Business: Innovative small molecules & biopharmaceuticals
Employees: >17,500
President: Elmar Schnee
Headquarters: Geneva, Switzerland
Key growth drivers:
4
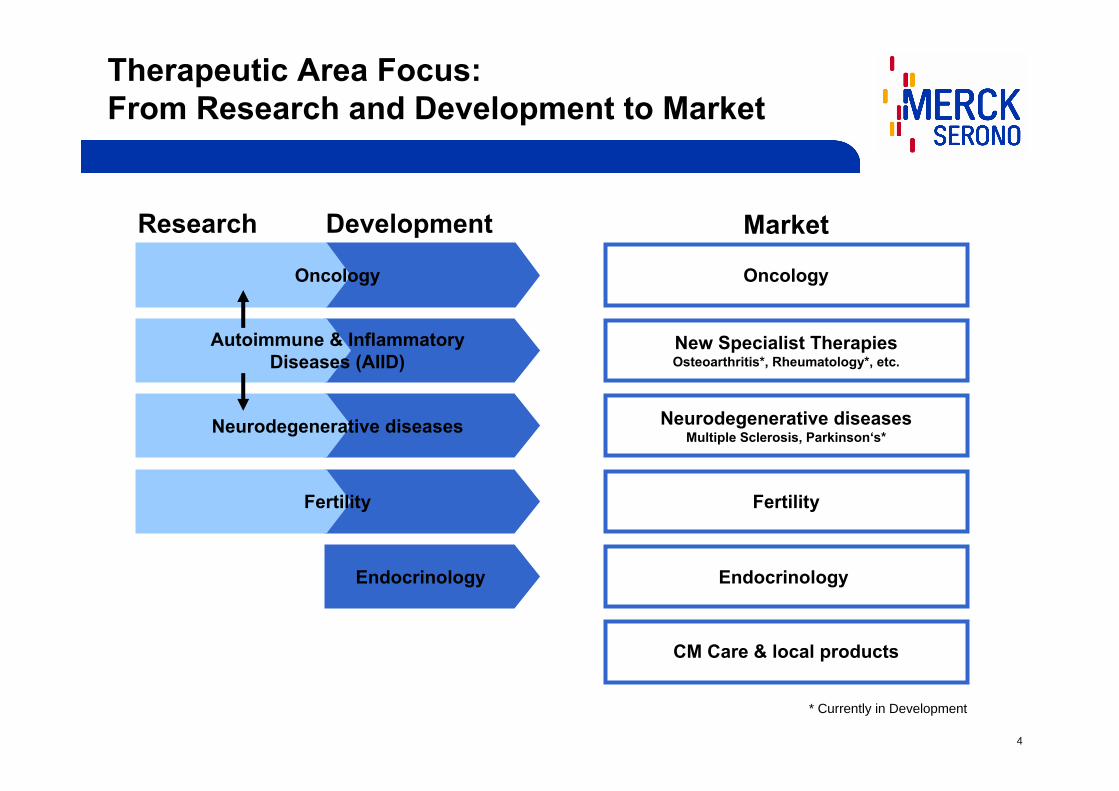
Research Development Market
Oncology
Endocrinology
* Currently in Development
Autoimmune & Inflammatory Diseases (AIID)
Fertility
Neurodegenerative diseases
Oncology
New Specialist TherapiesOsteoarthritis*, Rheumatology*, etc.
Neurodegenerative diseasesMultiple Sclerosis, Parkinson‘s*
Fertility
Endocrinology
CM Care & local products
Therapeutic Area Focus:From Research and Development to Market
5
Stratified Medicine is about Stratified Medicine is about adapting the treatmentadapting the treatment (molecule, dose, (molecule, dose, schedule,schedule,……) according to the patient) according to the patient’’s characteristics s characteristics
for better efficacy and less adverse events.for better efficacy and less adverse events.
Stratified Medicine: Definition
Personalized Medicine versus Stratified MedicinePatient sub-populationsIndividual patients,
e.g. cancer vaccine made from the patient’s tumor
6
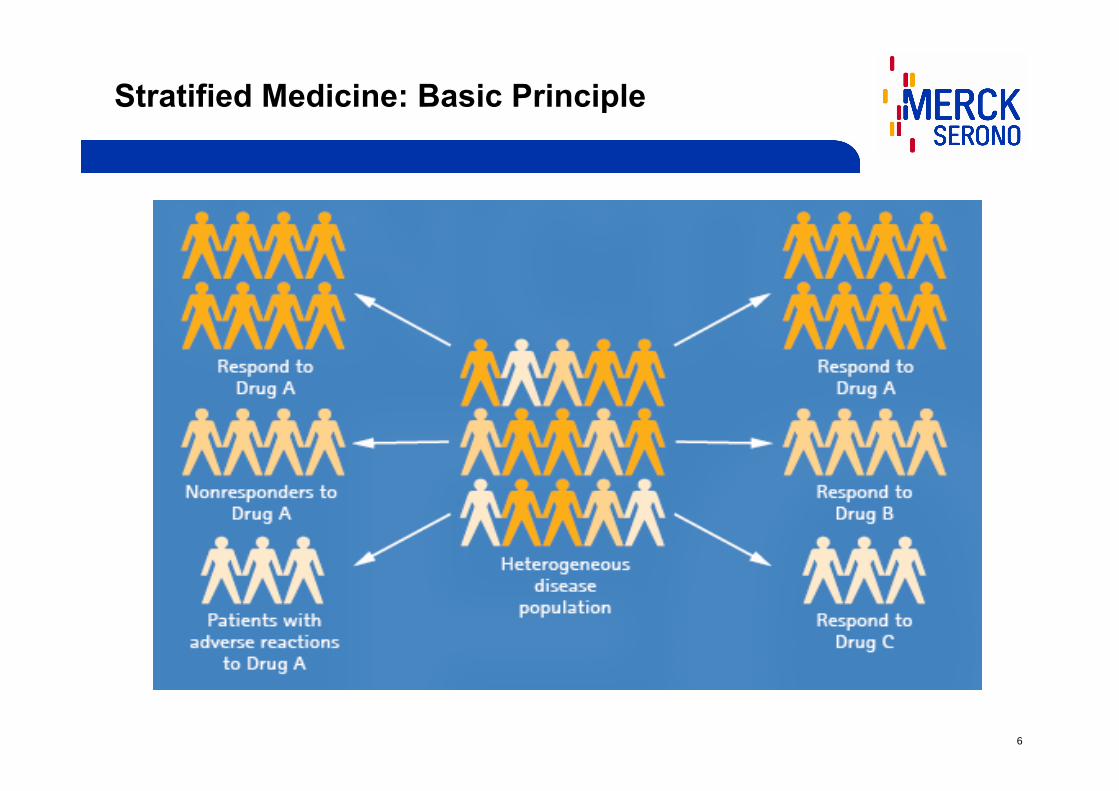
Stratified Medicine: Basic Principle
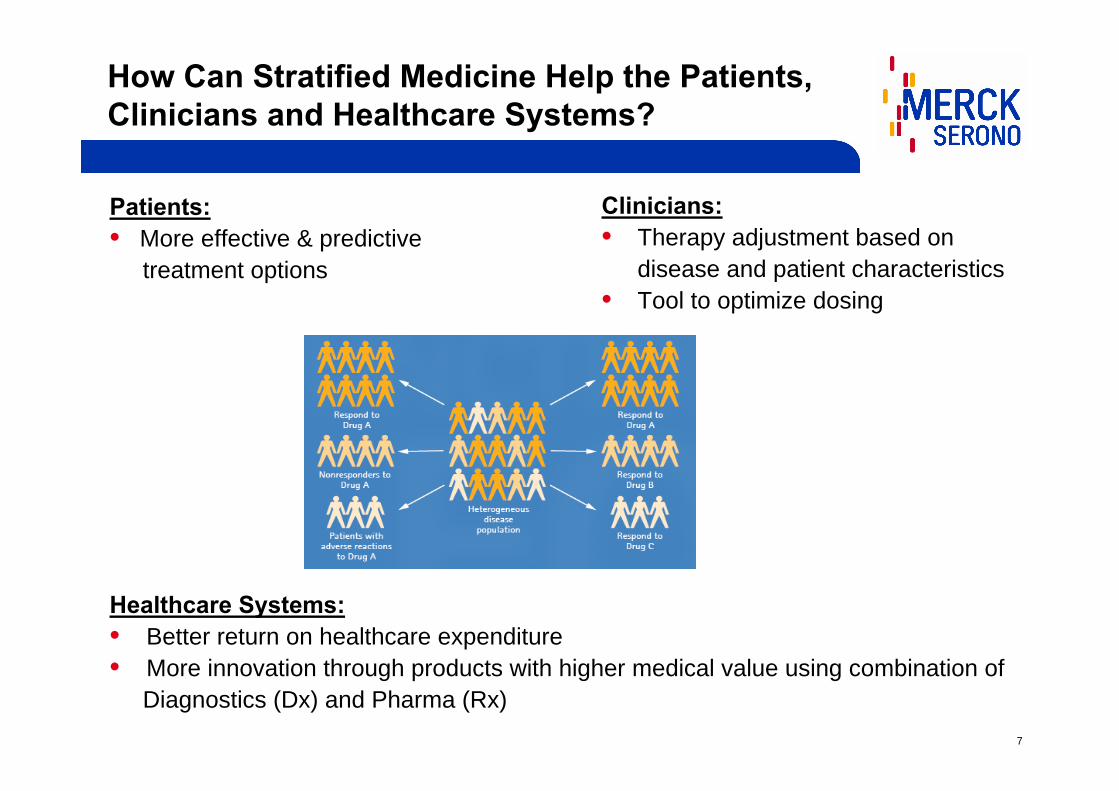
7
How Can Stratified Medicine Help the Patients, Clinicians and Healthcare Systems?
Clinicians:• Therapy adjustment based on
disease and patient characteristics• Tool to optimize dosing
Patients:• More effective & predictive
treatment options
Healthcare Systems:• Better return on healthcare expenditure• More innovation through products with higher medical value using combination of
Diagnostics (Dx) and Pharma (Rx)
8
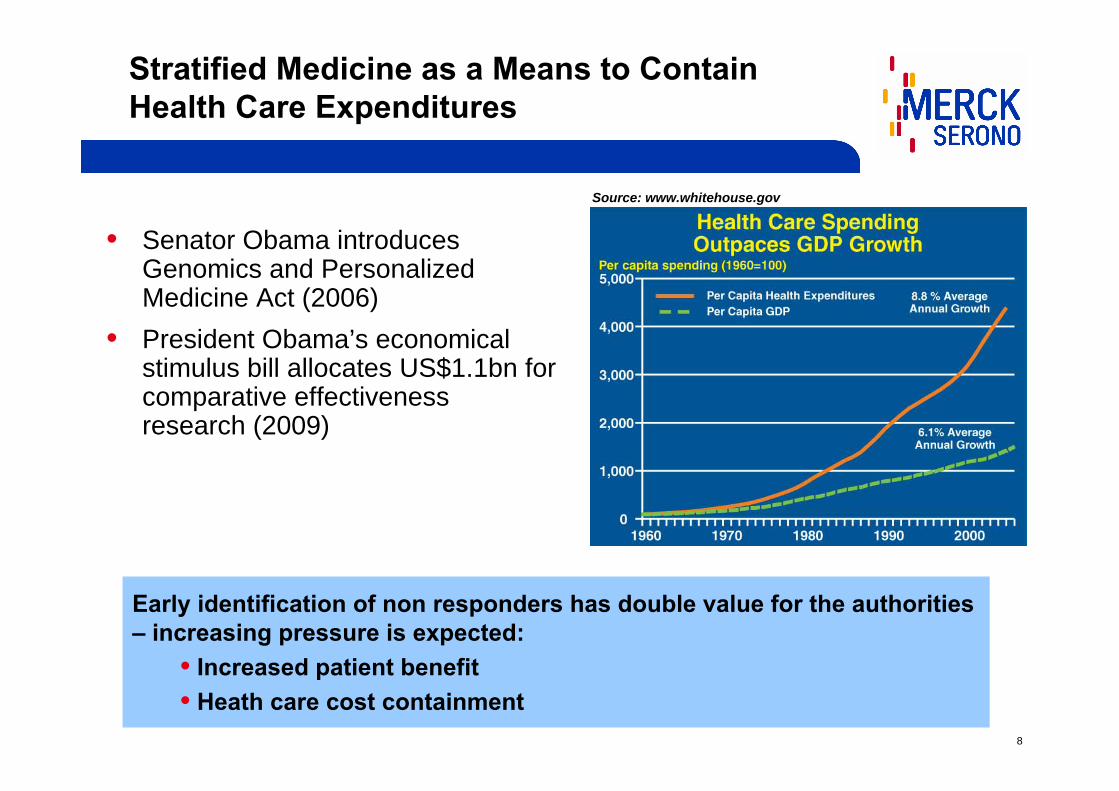
Stratified Medicine as a Means to ContainHealth Care Expenditures
• Senator Obama introducesGenomics and PersonalizedMedicine Act (2006)
• President Obama’s economicalstimulus bill allocates US$1.1bn for comparative effectivenessresearch (2009)
Source: www.whitehouse.gov
Early identification of non responders has double value for the authorities – increasing pressure is expected:
• Increased patient benefit• Heath care cost containment
9
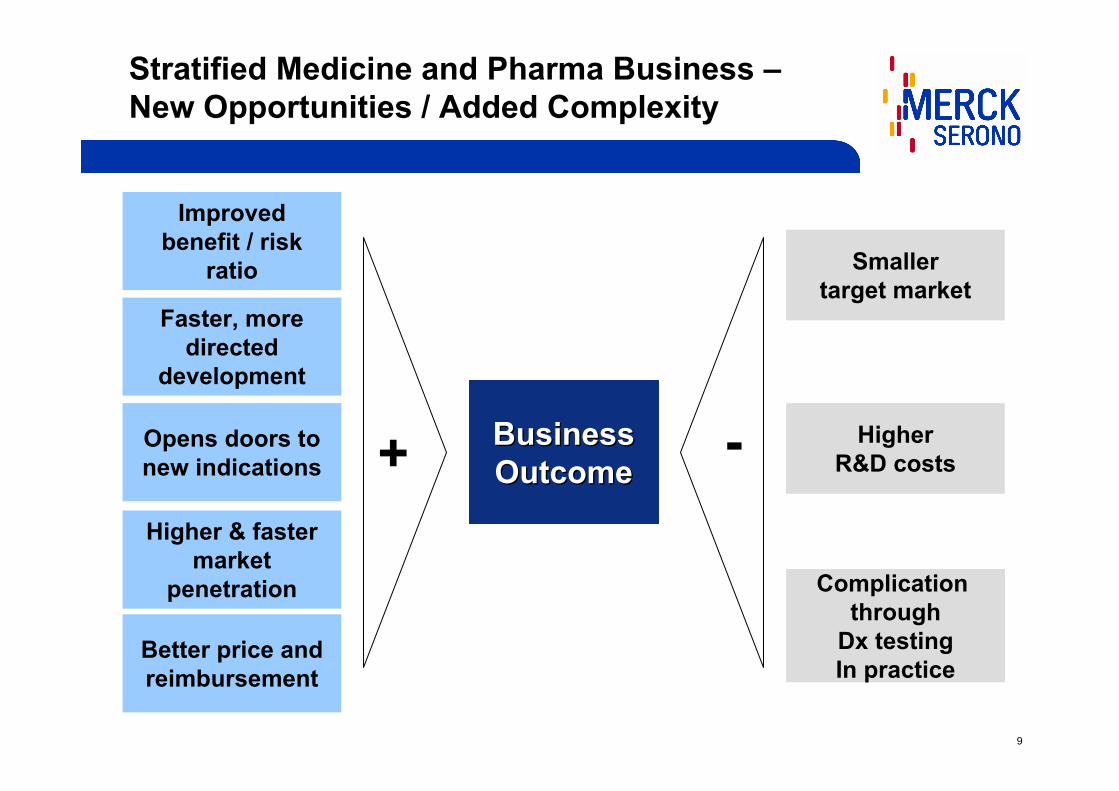
Stratified Medicine and Pharma Business –New Opportunities / Added Complexity
Improvedbenefit / risk
ratio
Opens doors tonew indications
Higher & fastermarket
penetration
Better price andreimbursement
Faster, more directed
development
Smallertarget market
HigherR&D costs
Complication through
Dx testingIn practice
BusinessBusinessOutcomeOutcome+
-
10
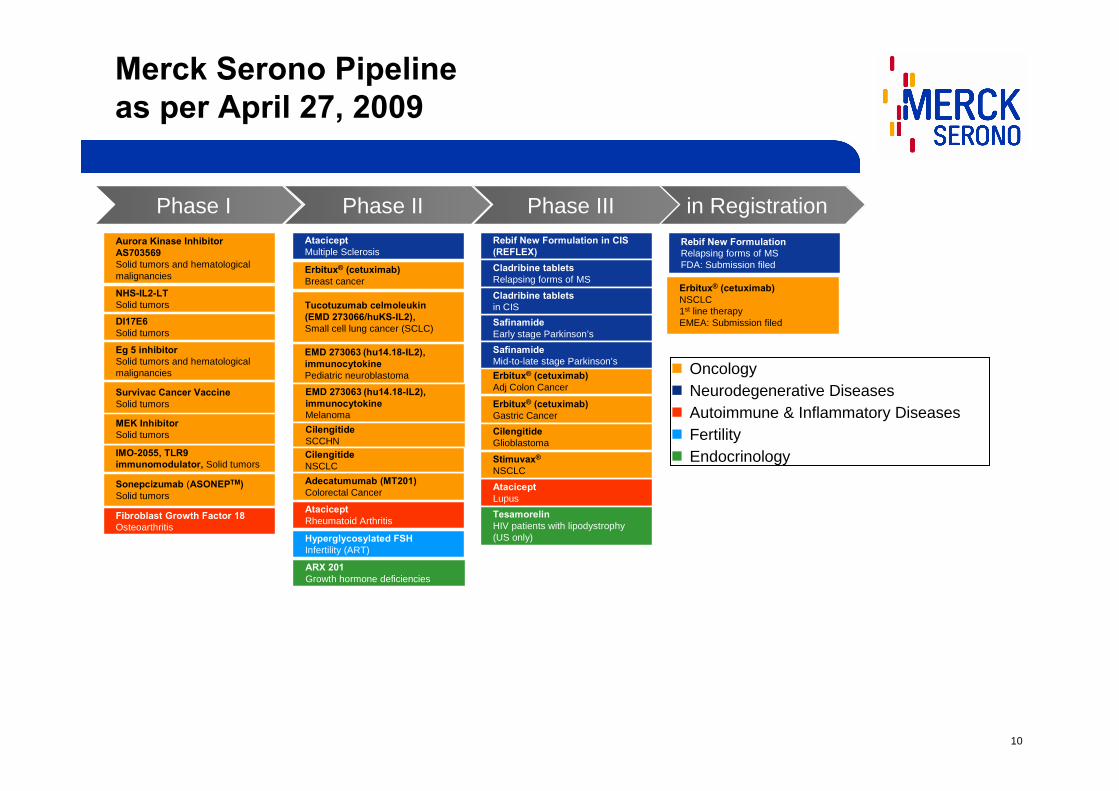
Merck Serono Pipelineas per April 27, 2009
Phase IIIPhase IIPhase I
ARX 201Growth hormone deficiencies
NHS-IL2-LTSolid tumors
DI17E6Solid tumors
Eg 5 inhibitorSolid tumors and hematologicalmalignancies
IMO-2055, TLR9 immunomodulator, Solid tumors
Survivac Cancer VaccineSolid tumors
Fibroblast Growth Factor 18Osteoarthritis
Aurora Kinase Inhibitor AS703569Solid tumors and hematologicalmalignancies
Adecatumumab (MT201)Colorectal Cancer
Tucotuzumab celmoleukin(EMD 273066/huKS-IL2), Small cell lung cancer (SCLC)
EMD 273063 (hu14.18-IL2),immunocytokinePediatric neuroblastoma
Hyperglycosylated FSHInfertility (ART)
EMD 273063 (hu14.18-IL2),immunocytokineMelanoma
AtaciceptRheumatoid Arthritis
Erbitux® (cetuximab)Breast cancer
AtaciceptMultiple Sclerosis
Erbitux® (cetuximab)Adj Colon Cancer
Erbitux® (cetuximab)Gastric Cancer
SafinamideEarly stage Parkinson’s
AtaciceptLupus
CilengitideGlioblastoma
Stimuvax®
NSCLC
SafinamideMid-to-late stage Parkinson’s
Rebif New Formulation in CIS (REFLEX)Cladribine tablets Relapsing forms of MS
in RegistrationPhase IIIPhase IIPhase I
TesamorelinHIV patients with lipodystrophy(US only)
Rebif New Formulation Relapsing forms of MSFDA: Submission filed
MEK InhibitorSolid tumors
Cladribine tablets in CIS
CilengitideSCCHN
Sonepcizumab (ASONEPTM)Solid tumors
Erbitux® (cetuximab)NSCLC1st line therapyEMEA: Submission filed
CilengitideNSCLC
Phase IIIPhase IIPhase I
ARX 201Growth hormone deficiencies
NHS-IL2-LTSolid tumors
DI17E6Solid tumors
Eg 5 inhibitorSolid tumors and hematologicalmalignancies
IMO-2055, TLR9 immunomodulator, Solid tumors
Survivac Cancer VaccineSolid tumors
Fibroblast Growth Factor 18Osteoarthritis
Aurora Kinase Inhibitor AS703569Solid tumors and hematologicalmalignancies
Adecatumumab (MT201)Colorectal Cancer
Tucotuzumab celmoleukin(EMD 273066/huKS-IL2), Small cell lung cancer (SCLC)
EMD 273063 (hu14.18-IL2),immunocytokinePediatric neuroblastoma
Hyperglycosylated FSHInfertility (ART)
EMD 273063 (hu14.18-IL2),immunocytokineMelanoma
AtaciceptRheumatoid Arthritis
Erbitux® (cetuximab)Breast cancer
AtaciceptMultiple Sclerosis
Erbitux® (cetuximab)Adj Colon Cancer
Erbitux® (cetuximab)Gastric Cancer
SafinamideEarly stage Parkinson’s
AtaciceptLupus
CilengitideGlioblastoma
Stimuvax®
NSCLC
SafinamideMid-to-late stage Parkinson’s
Rebif New Formulation in CIS (REFLEX)Cladribine tablets Relapsing forms of MS
in RegistrationPhase IIIPhase IIPhase I
TesamorelinHIV patients with lipodystrophy(US only)
Rebif New Formulation Relapsing forms of MSFDA: Submission filed
MEK InhibitorSolid tumors
Cladribine tablets in CIS
CilengitideSCCHN
Sonepcizumab (ASONEPTM)Solid tumors
Erbitux® (cetuximab)NSCLC1st line therapyEMEA: Submission filed
CilengitideNSCLC
OncologyNeurodegenerative DiseasesAutoimmune & Inflammatory DiseasesFertilityEndocrinology

11
Phase IIIPhase IIPhase I
ARX 201Growth hormone deficiencies
NHS-IL2-LTSolid tumors
DI17E6Solid tumors
Eg 5 inhibitorSolid tumors and hematologicalmalignancies
IMO-2055, TLR9 immunomodulator, Solid tumors
Survivac Cancer VaccineSolid tumors
Fibroblast Growth Factor 18Osteoarthritis
Aurora Kinase Inhibitor AS703569Solid tumors and hematologicalmalignancies
Adecatumumab (MT201)Colorectal Cancer
Tucotuzumab celmoleukin(EMD 273066/huKS-IL2), Small cell lung cancer (SCLC)
EMD 273063 (hu14.18-IL2),immunocytokinePediatric neuroblastoma
Hyperglycosylated FSHInfertility (ART)
EMD 273063 (hu14.18-IL2),immunocytokineMelanoma
AtaciceptRheumatoid Arthritis
Erbitux® (cetuximab)Breast cancer
AtaciceptMultiple Sclerosis
Erbitux® (cetuximab)Adj Colon Cancer
Erbitux® (cetuximab)Gastric Cancer
SafinamideEarly stage Parkinson’s
AtaciceptLupus
CilengitideGlioblastoma
Stimuvax®
NSCLC
SafinamideMid-to-late stage Parkinson’s
Rebif New Formulation in CIS (REFLEX)Cladribine tablets Relapsing forms of MS
in RegistrationPhase IIIPhase IIPhase I
TesamorelinHIV patients with lipodystrophy(US only)
Rebif New Formulation Relapsing forms of MSFDA: Submission filed
MEK InhibitorSolid tumors
Cladribine tablets in CIS
CilengitideSCCHN
Sonepcizumab (ASONEPTM)Solid tumors
Erbitux® (cetuximab)NSCLC1st line therapyEMEA: Submission filed
CilengitideNSCLC
Phase IIIPhase IIPhase I
ARX 201Growth hormone deficiencies
NHS-IL2-LTSolid tumors
DI17E6Solid tumors
Eg 5 inhibitorSolid tumors and hematologicalmalignancies
IMO-2055, TLR9 immunomodulator, Solid tumors
Survivac Cancer VaccineSolid tumors
Fibroblast Growth Factor 18Osteoarthritis
Aurora Kinase Inhibitor AS703569Solid tumors and hematologicalmalignancies
Adecatumumab (MT201)Colorectal Cancer
Tucotuzumab celmoleukin(EMD 273066/huKS-IL2), Small cell lung cancer (SCLC)
EMD 273063 (hu14.18-IL2),immunocytokinePediatric neuroblastoma
Hyperglycosylated FSHInfertility (ART)
EMD 273063 (hu14.18-IL2),immunocytokineMelanoma
AtaciceptRheumatoid Arthritis
Erbitux® (cetuximab)Breast cancer
AtaciceptMultiple Sclerosis
Erbitux® (cetuximab)Adj Colon Cancer
Erbitux® (cetuximab)Gastric Cancer
SafinamideEarly stage Parkinson’s
AtaciceptLupus
CilengitideGlioblastoma
Stimuvax®
NSCLC
SafinamideMid-to-late stage Parkinson’s
Rebif New Formulation in CIS (REFLEX)Cladribine tablets Relapsing forms of MS
in RegistrationPhase IIIPhase IIPhase I
TesamorelinHIV patients with lipodystrophy(US only)
Rebif New Formulation Relapsing forms of MSFDA: Submission filed
MEK InhibitorSolid tumors
Cladribine tablets in CIS
CilengitideSCCHN
Sonepcizumab (ASONEPTM)Solid tumors
Erbitux® (cetuximab)NSCLC1st line therapyEMEA: Submission filed
CilengitideNSCLC
Biomarker and or stratification activities
OncologyNeurodegenerative DiseasesAutoimmune & Inflammatory DiseasesFertilityEndocrinology
v
Merck Serono Pipelineas per April 27, 2009
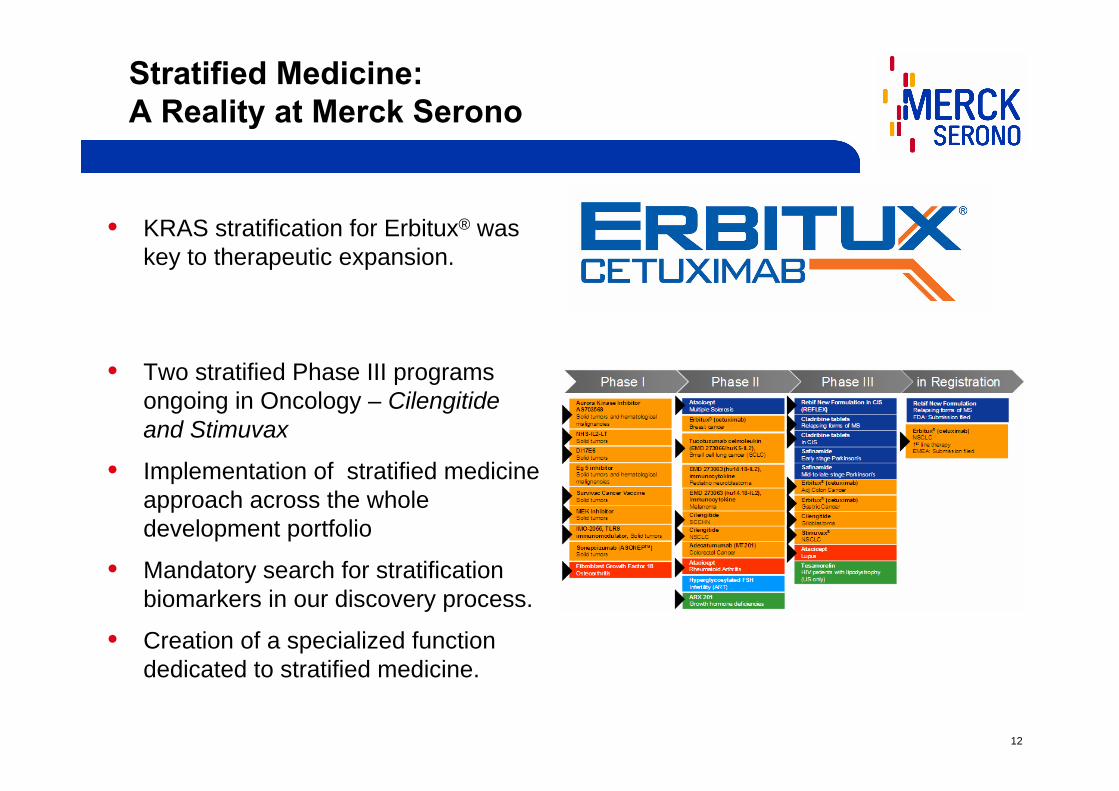
Stratification is an important part of the Merck Serono strategy.Over 60% of our portfolio include Biomarker programs
(predictive, mechanistic, surrogates).
12
Stratified Medicine: A Reality at Merck Serono
• KRAS stratification for Erbitux® was key to therapeutic expansion.
• Two stratified Phase III programs ongoing in Oncology – Cilengitideand Stimuvax
• Implementation of stratified medicine approach across the whole development portfolio
• Mandatory search for stratification biomarkers in our discovery process.
• Creation of a specialized function dedicated to stratified medicine.
13
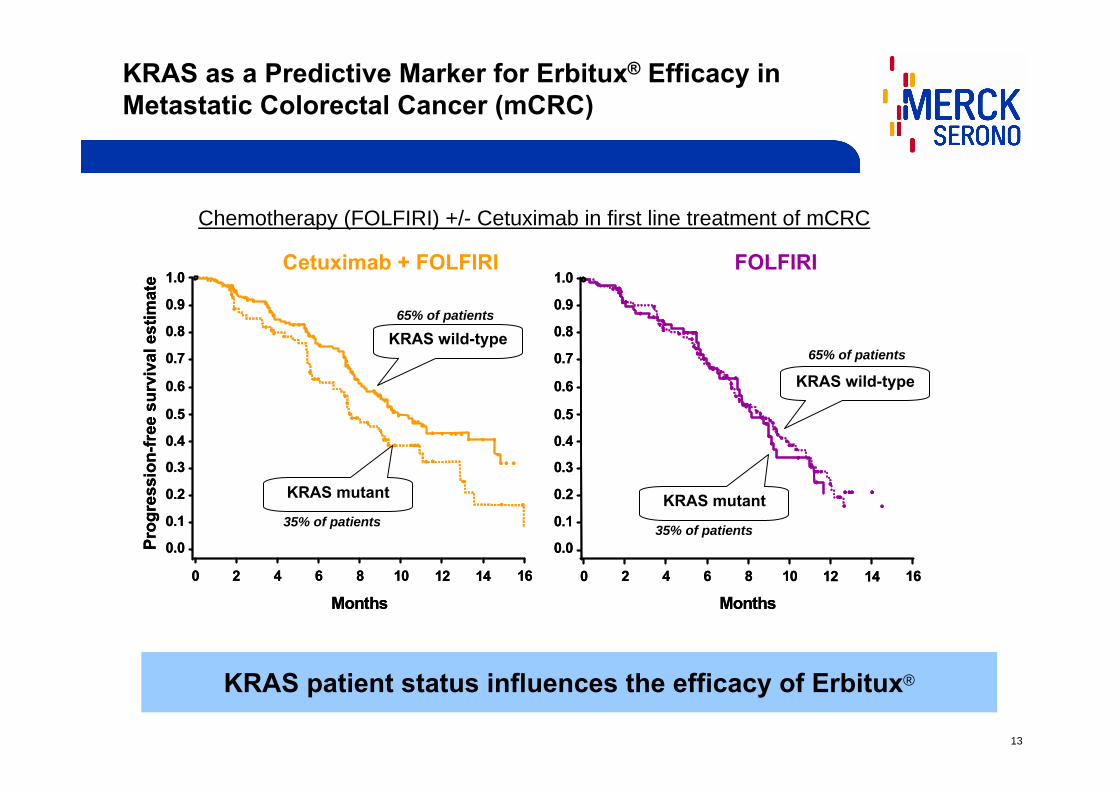
KRAS as a Predictive Marker for Erbitux® Efficacy in Metastatic Colorectal Cancer (mCRC)
KRAS patient status influences the efficacy of Erbitux®
0.5
1.0
0.4
0.3
0.2
0.1
0.0
0.6
0.7
0.8
0.9
80 2 4 6 10 16
Prog
ress
ion-
free
sur
viva
l est
imat
e
Months12 14
0.5
1.0
0.4
0.3
0.2
0.1
0.0
0.6
0.7
0.8
0.9
80 2 4 6 10 16
Prog
ress
ion-
free
sur
viva
l est
imat
e
Months12 14
0.5
1.0
0.4
0.3
0.2
0.1
0.0
0.6
0.7
0.8
0.9
Months80 2 4 6 10 1612 14
0.5
1.0
0.4
0.3
0.2
0.1
0.0
0.6
0.7
0.8
0.9
Months80 2 4 6 10 1612 14
Cetuximab + FOLFIRI FOLFIRI
KRAS wild-type
KRAS wild-type
KRAS mutant KRAS mutant
Chemotherapy (FOLFIRI) +/- Cetuximab in first line treatment of mCRC
65% of patients
65% of patients
35% of patients35% of patients
14
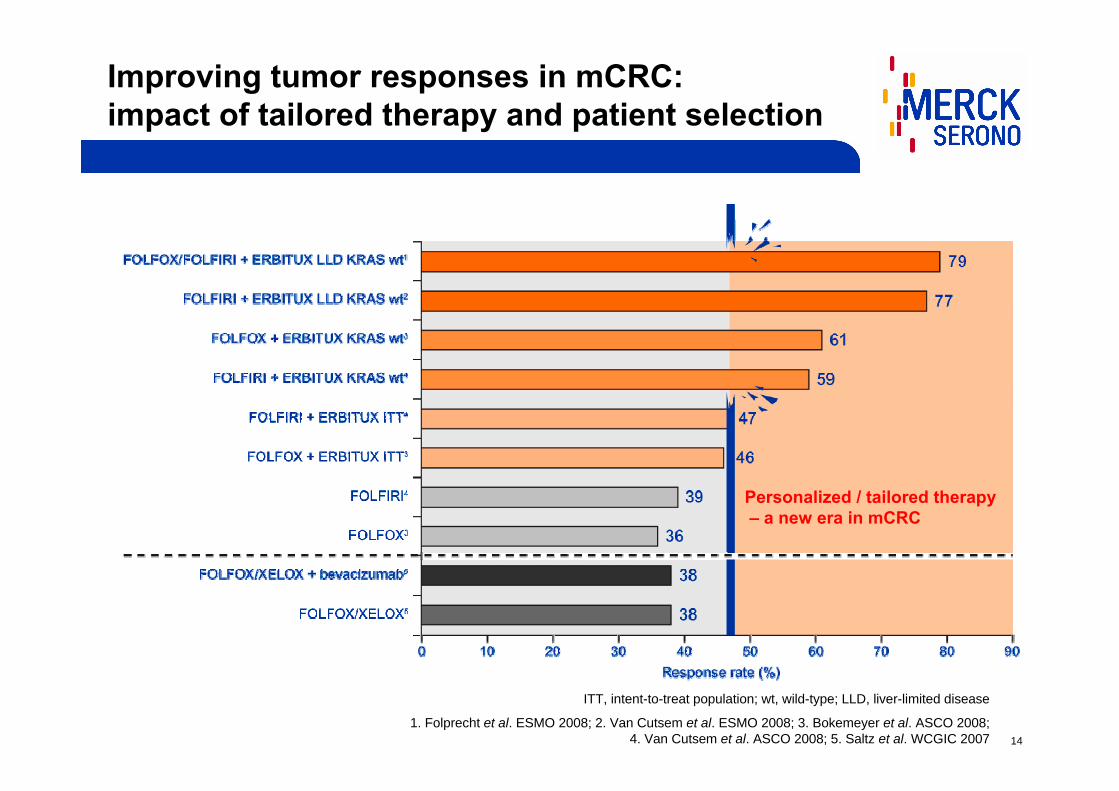
Improving tumor responses in mCRC: impact of tailored therapy and patient selection
ITT, intent-to-treat population; wt, wild-type; LLD, liver-limited disease
1. Folprecht et al. ESMO 2008; 2. Van Cutsem et al. ESMO 2008; 3. Bokemeyer et al. ASCO 2008; 4. Van Cutsem et al. ASCO 2008; 5. Saltz et al. WCGIC 2007
Personalized / tailored therapy– a new era in mCRC

15
Benefit-effort ratio
100% pts treated with non-tailored therapyIdentified 60% pts (KRAS wt) treated with tailored therapy
Target specific patient group (KRAS wt) No indicators to select patients
Maximize success in clinical studiesGood clinical benefit in stratified patients Avoid unnecessary adverse effectsEfficient from health economics perspective
Variable success in clinical studiesVariable clinical benefit in allcomersRisk of unnecessary adverse effectsInefficient from health economics perspective

16
Extension of mCRC Indication to 1st Line withKRAS Stratification
11stst lineline74,200 patients74,200 patients
22ndnd lineline32,200 patients32,200 patients
33rdrd lineline10,200 patients10,200 patients
Treatment duration
32 weeks20 weeks16 weeks
KRAS wild-type48,230 patients
KRAS wild-type 20,930 patients
KRAS wild-type6,630 patients
KRAS wild-type65%
*Data for biggest 5 countries in Europe, Source: OncFoundation2007 projections for 2008
Treating 2nd and 3rd line,both KRAS wild-type and mutant:Market = 807,200 weeks treatment
Treating 1st line,KRAS wild-type only:
Market = 1,543,360 weeks treatment
TreatmentTreatmentlineline
Bigger market enabled by stratificationHigher penetration due to improved efficacy
KRAS mutant25,970 patients
KRAS mutant 11.270 patients
KRAS mutant3,570 patients
KRAS mutant35%

17
1 June 2009: Breakthrough for Erbitux in the UK ─ NICE recommendation thanks to KRAS
85 pieces of coverage for NICE (11 in major newspapers/newswires)

18
Cilengitide in Glioblastoma
• Glioblastoma is a rare tumor, difficult to treat.
• The methylation of the MGMT* gene promoter is a potential stratification marker.
• Increased likelihood to succeed in Phase III using MGMT stratification.
Stratified medicine helps to meet unmet medical needs and to access additional indications
*O-Methylguanine-DNA Methyltransferase

19
Study Conduct & BM Logistics
Biomarker Technologies
Consequences of Stratified Medicine Implementation on Technology ManagementNew capabilities → New complexities
Drug Development
Clinical Study Design
20
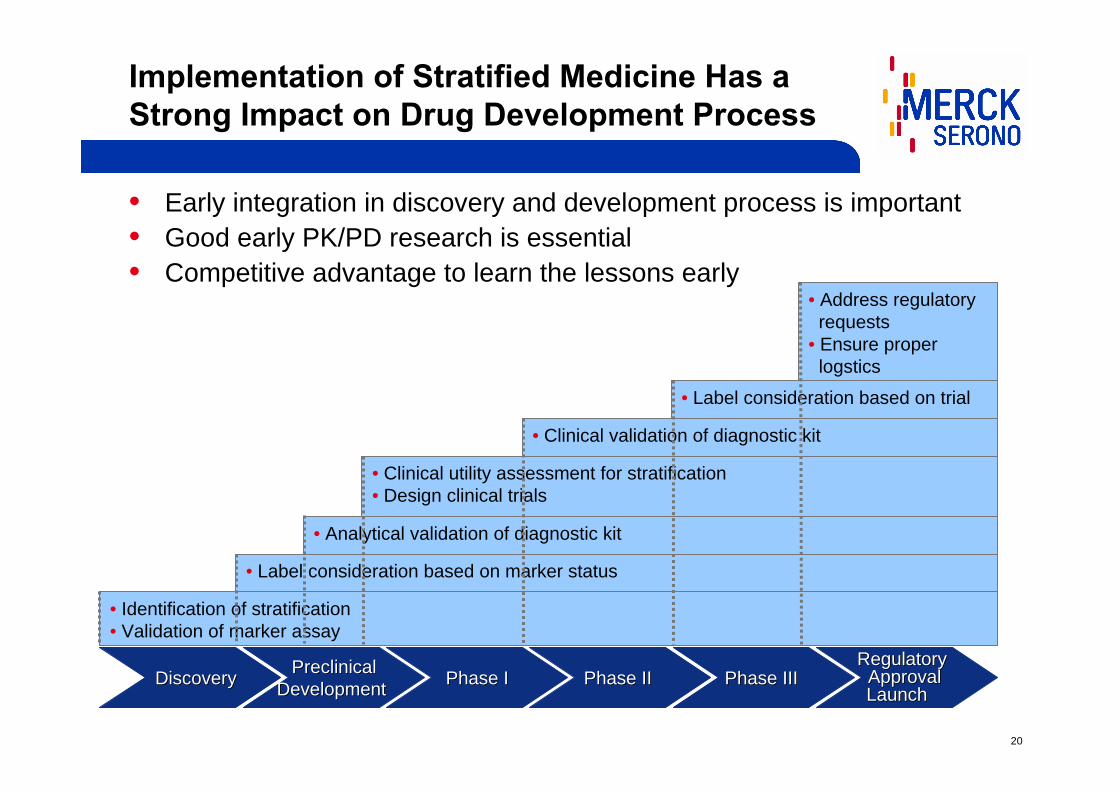
Implementation of Stratified Medicine Has a Strong Impact on Drug Development Process
• Early integration in discovery and development process is important• Good early PK/PD research is essential• Competitive advantage to learn the lessons early
DiscoveryDiscovery PreclinicalPreclinicalDevelopmentDevelopment Phase IPhase I Phase IIPhase II Phase IIIPhase III
RegulatoryRegulatoryApprovalApprovalLaunchLaunch
• Identification of stratification• Validation of marker assay
• Label consideration based on marker status
• Analytical validation of diagnostic kit
• Clinical utility assessment for stratification• Design clinical trials
• Clinical validation of diagnostic kit
• Label consideration based on trial
• Address regulatory requests
• Ensure properlogstics
21
Requirements for Stratification Kits in the Pharma Business
• Technical reliability:– Selective– Sensitive– Reproducible– Validated in clinical setting– Short turn-around
• Market access:– Properly distributed– Technically user-friendly– Financially affordable
Conditions for Conditions for ““good stratification kitsgood stratification kits””from the Rx standpoints:from the Rx standpoints:
Alignment of Rx and Dx is important
22
Are the Current Rx/Dx Business ModelsChallenged in the Context of Stratified Medicine?
• Price is set according to the medical value
Innovative drugs increasing the response rate - bringing real added benefit to the patients - will enjoy higher reimbursement
• Price is set according to the product cost
Innovative genotyping kit increasing the response rate will be reimbursed at the level of other genotyping methods
Will Dx benefit increasingly from value-based recognition?
Rx reimbursement:Value-based system
Dx reimbursement:Cost-based system
23
Dx and Rx Interactions
• Dx develops stratification markers for marketed drugs without Rx partnership
• Strong impact on Rx business since drug price is unlikely to be re-negotiable
• Kit development risk shouldered by Dx
• Risk of double marginalization
• Dx/Rx misalignment might be detrimental for patients benefit
• Dx co-develops stratification markers with Rx
• Higher Dx price negotiable at launch
• Shared development risk, mainly covered by Rx
• Profit sharing & optimization
• Aligned commercialization efforts -Best medical benefit for patients
Stratified Medicine might result in a new Dx/Rx symbiosis.
Invasive model Collaborative model
Two extreme models:
24
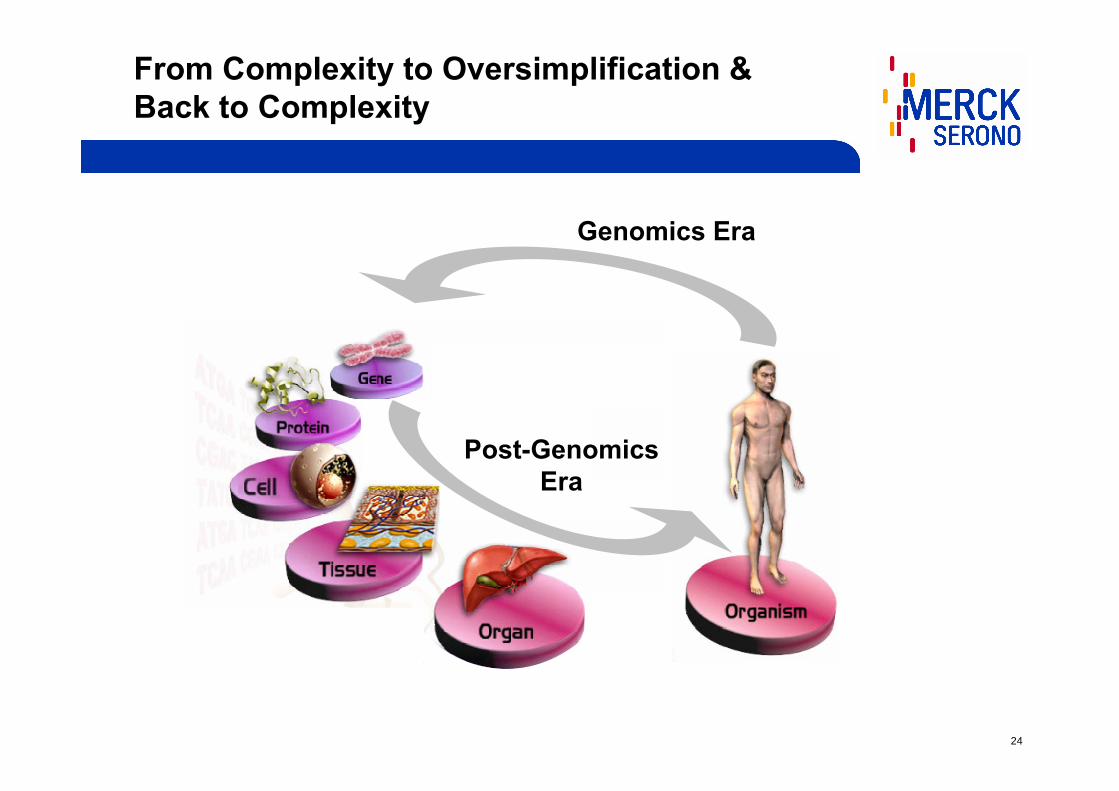
From Complexity to Oversimplification & Back to Complexity
Genomics Era
Post-GenomicsEra
25
Contact information
Dr. Thomas Kornek℡ +49 6151 72-7434Claudia Nickolaus℡ +49 6151 72-2584Alessandra HeinzAssistant Investor Relations℡ +49 6151 72-3321
Merck KGaAInvestor RelationsFrankfurter Str. 25064293 DarmstadtGermanyFax: +49 6151 [email protected]
Thank you for yourkind attention!
Further Contact







