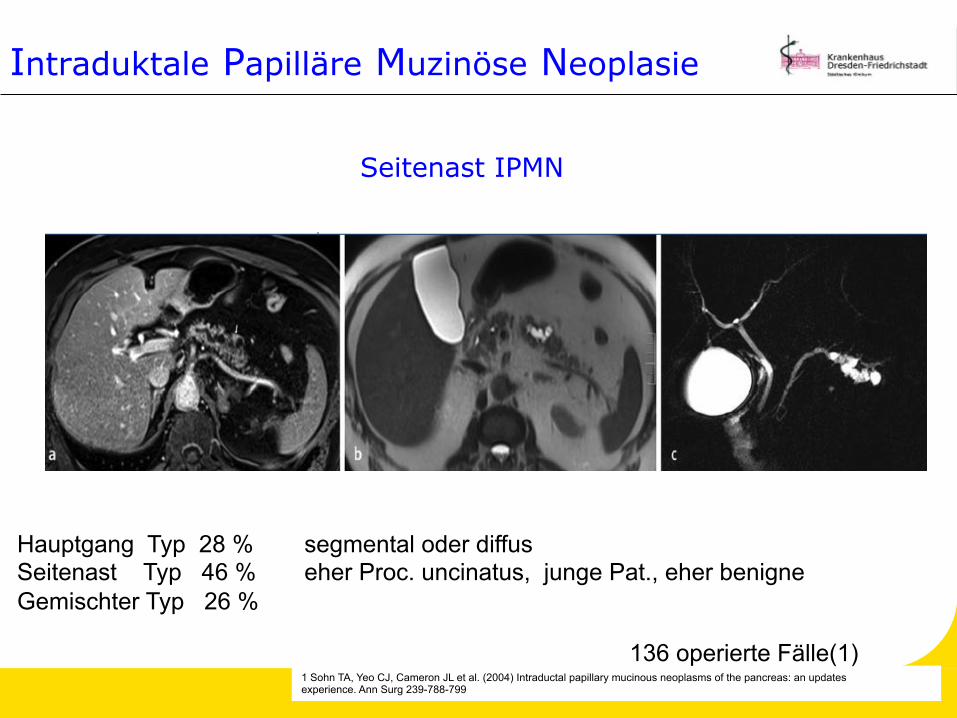
Hauptgang Typ 28 % segmental oder diffus Seitenast Typ 46 % eher Proc. uncinatus, junge Pat., eher benigne Gemischter Typ 26 %
1 Sohn TA, Yeo CJ, Cameron JL et al. (2004) Intraductal papillary mucinous neoplasms of the pancreas: an updates experience. Ann Surg 239-788-799
136 operierte Fälle(1)
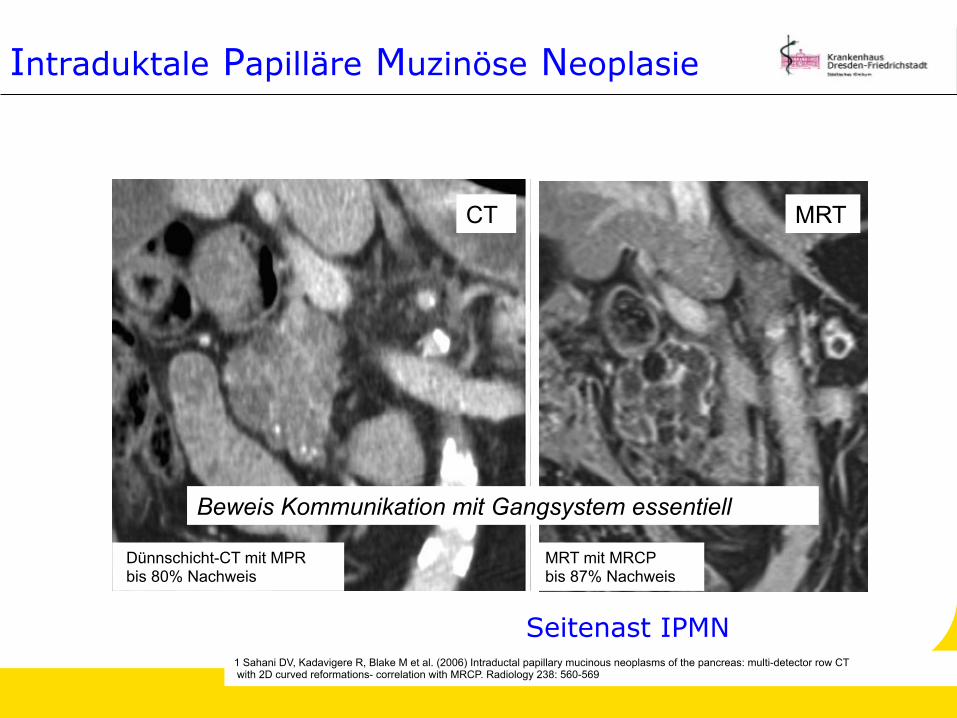
Seitenast IPMN
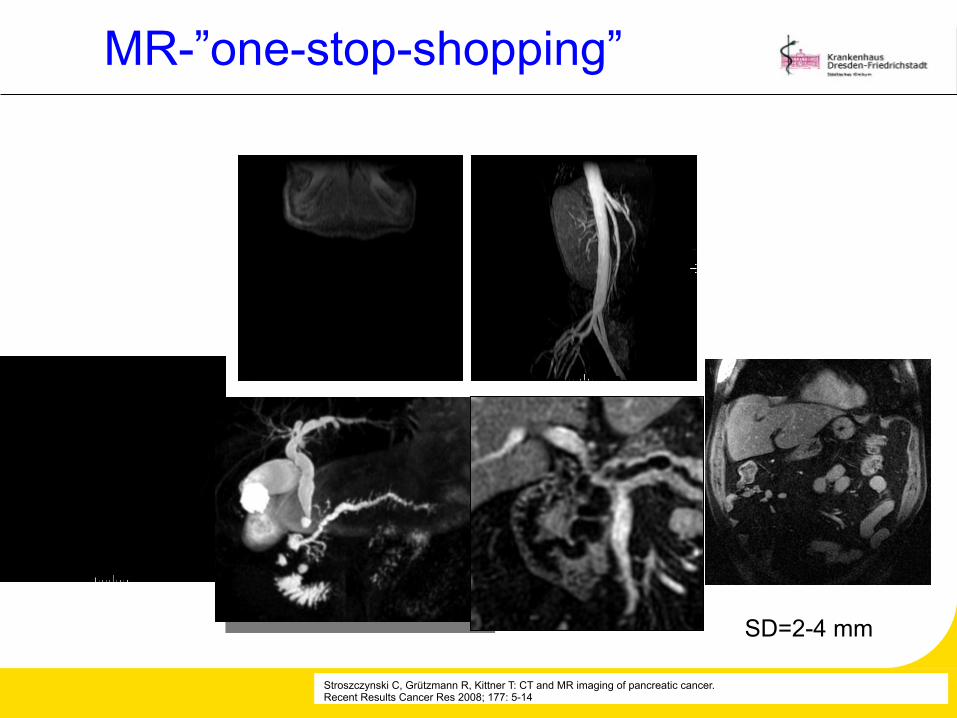
Dünnschicht-CT mit MPR bis 80% Nachweis
1 Sahani DV, Kadavigere R, Blake M et al. (2006) Intraductal papillary mucinous neoplasms of the pancreas: multi-detector row CT with 2D curved reformations- correlation with MRCP. Radiology 238: 560-569
Seitenast IPMN
CT
Intraduktale Papilläre Muzinöse Neoplasie
MRT
MRT mit MRCP bis 87% Nachweis
Beweis Kommunikation mit Gangsystem essentiell
Seitenast IPMN ?
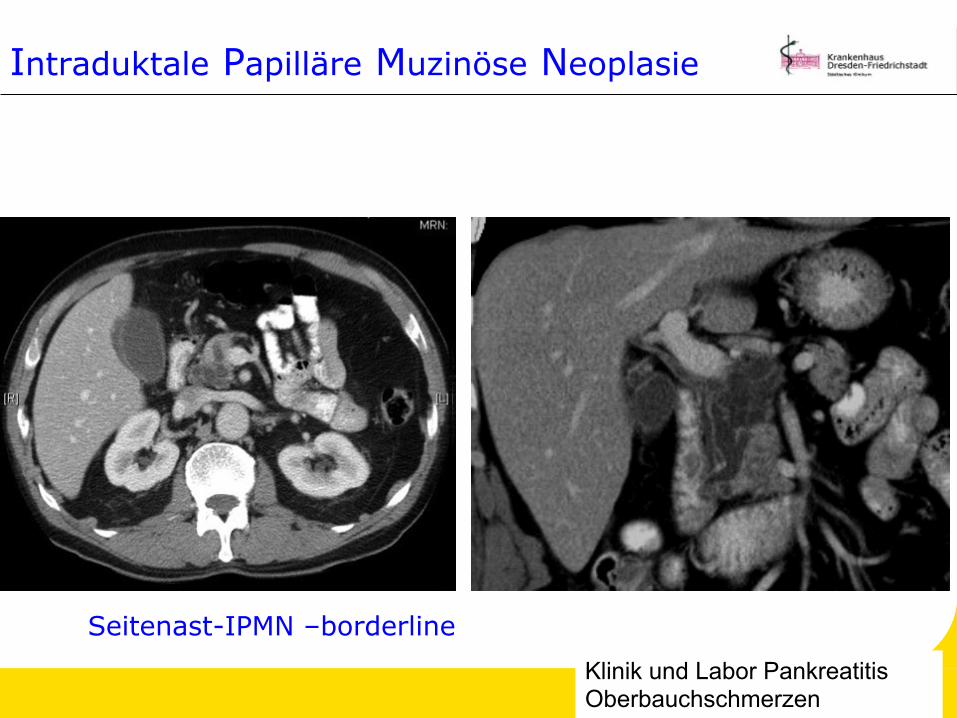
Seitenast-IPMN –borderline Klinik und Labor Pankreatitis Oberbauchschmerzen
Intraduktale Papilläre Muzinöse Neoplasie
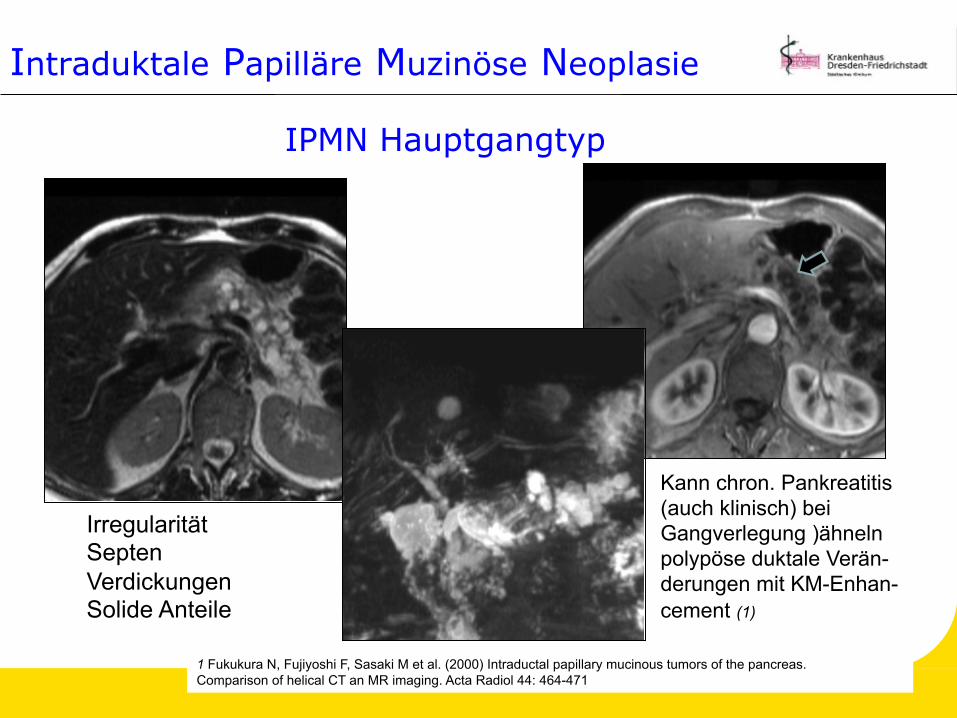
IPMN Hauptgangtyp
Irregularität Septen Verdickungen Solide Anteile
Kann chron. Pankreatitis (auch klinisch) bei Gangverlegung )ähneln polypöse duktale Verän- derungen mit KM-Enhan- cement (1)
1 Fukukura N, Fujiyoshi F, Sasaki M et al. (2000) Intraductal papillary mucinous tumors of the pancreas. Comparison of helical CT an MR imaging. Acta Radiol 44: 464-471
Intraduktale Papilläre Muzinöse Neoplasie
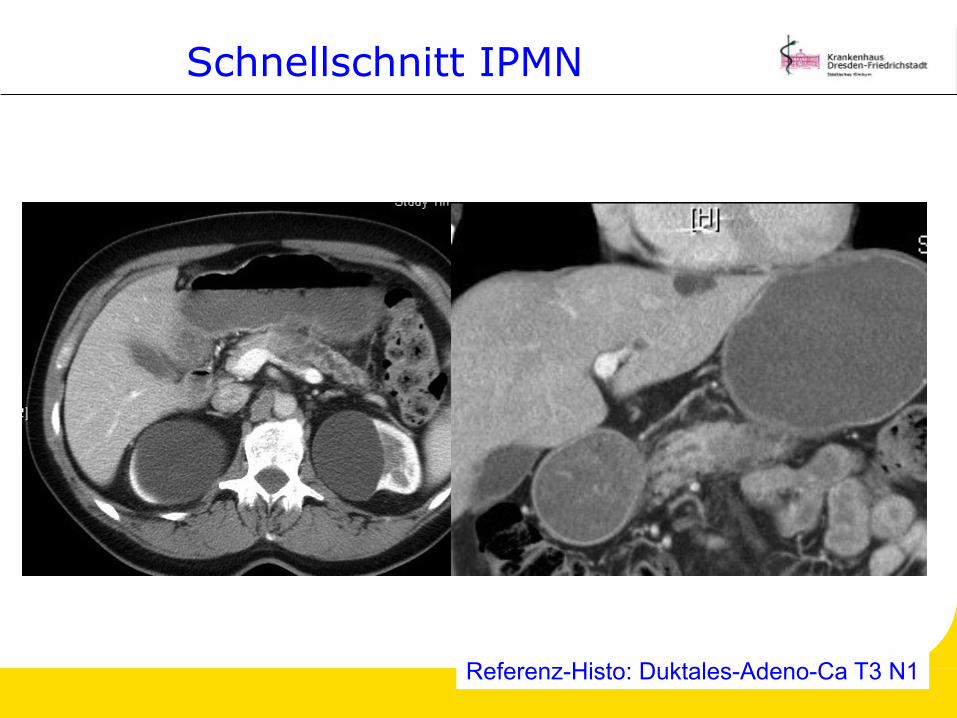
Schnellschnitt IPMN
Referenz-Histo: Duktales-Adeno-Ca T3 N1
Gutartig 2,6 cm Durchmesser Borderline Maligne Tumoren Carcinoma in situ 27% (4,7 cm Durchmesser, Hauptgang weiter als benigne, Gallengang dilatiert)
Invasives Karzinom 40% (muzinös, duktal) werden solider
Klöppel G (1998) Clinicopathologic view of intraductal papillary-mucinous tumor of the pancreas. Hepatogastroenterology 45: 1981-1985
Intraduktale Papilläre Muzinöse Neoplasie
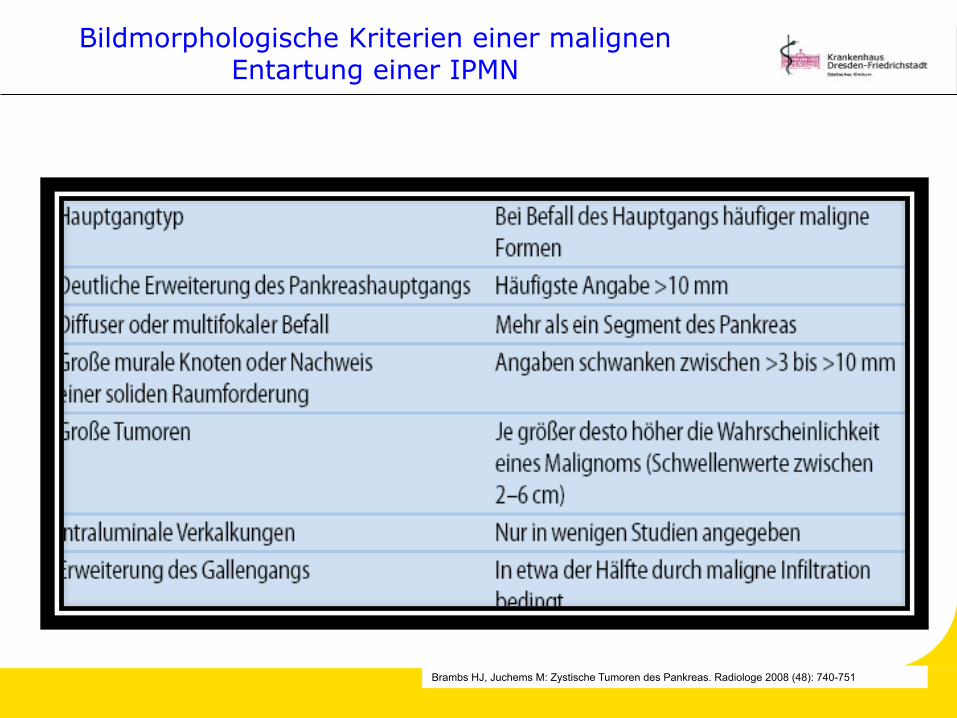
Bildmorphologische Kriterien einer malignen Entartung einer IPMN
Tumoren ohne Verbindung mit dem Gangsystem, die schleimbildendes Epithel und häufig ein ovarienartiges Stroma aufweisen (1) fast ausschließlich weibliche Patienten (M:F=1:9) (2) meist solitär dickwandige bzw. gekammerte Zysten meist größer und Druckschmerzen, nur 25% symptomlos Tumorgröße > 6 cm und Knotennachweis korreliert mit Entartungsrisiko (3)
(17,5% Ca, 10,5% borderline, 70% Adenom. Crippa S et al., Ann Surg, 2008) 95% in Korpus und Schwanz
Hämorrhagie stark hinweisend auf MZN Ddx monozystische Tumore vs. Pseudozysten schwer (4)
1 Zamboni G, Scarpa A, Bogina G et al. (1999 ) Mucinous cystic tumors of the pancreas: clinicopathological features, prognosis, and relationship to other mucinous cystic tumors. Am J Surg Pathol 23: 410-422
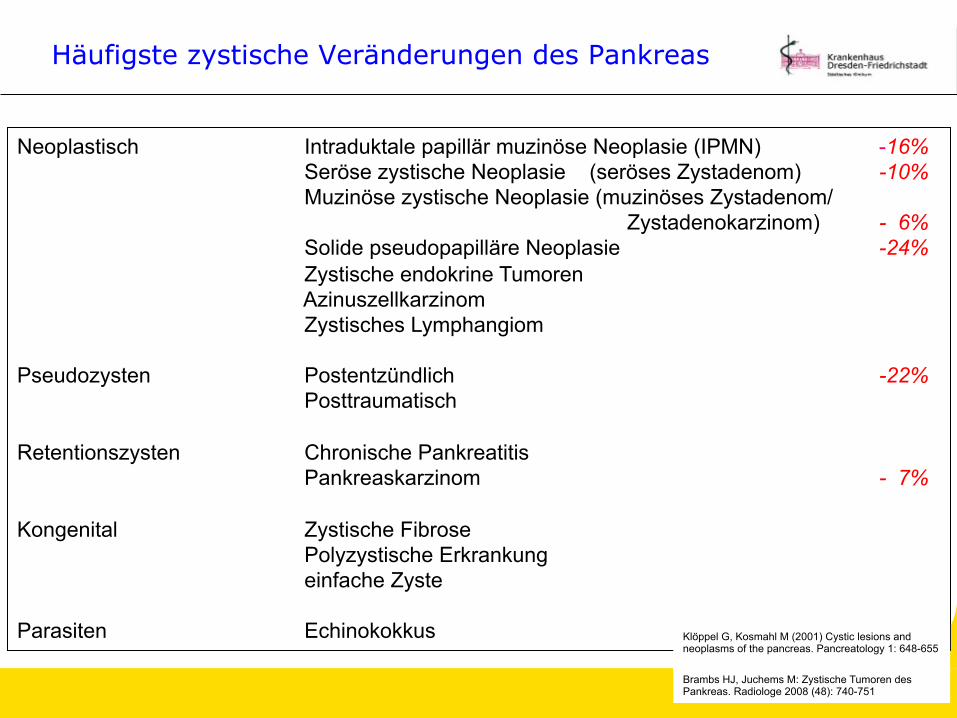
2 Klöppel G, Kosmahl M (2001) Cystic lesions and neoplasms of the pancreas. Pancreatology 1: 648-655
3 Thompson LD, Becker RC, Przygodzky et al. (1999) Mucinous cystic neoplasms (mucinous cystadenocarcinoma of low-grade malignant potential )of the pancreas: a clinicopathological study of 130 casesAm J Surg Pathol 23: 1-16
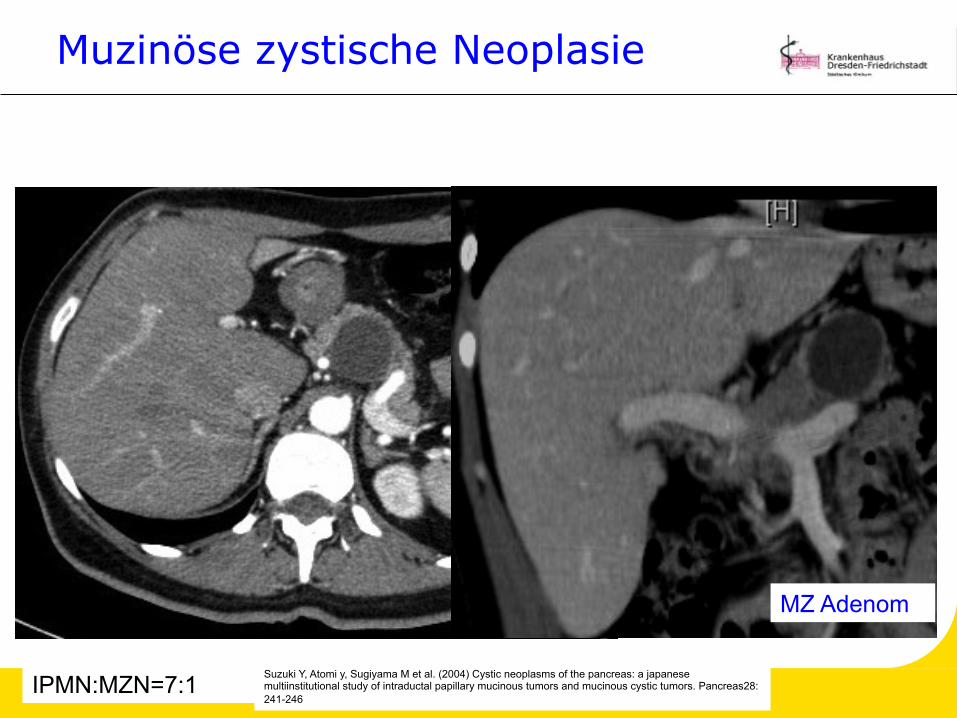
Muzinöse zystische Neoplasie
MZ Adenom
IPMN:MZN=7:1 Suzuki Y, Atomi y, Sugiyama M et al. (2004) Cystic neoplasms of the pancreas: a japanese multiinstitutional study of intraductal papillary mucinous tumors and mucinous cystic tumors. Pancreas28: 241-246
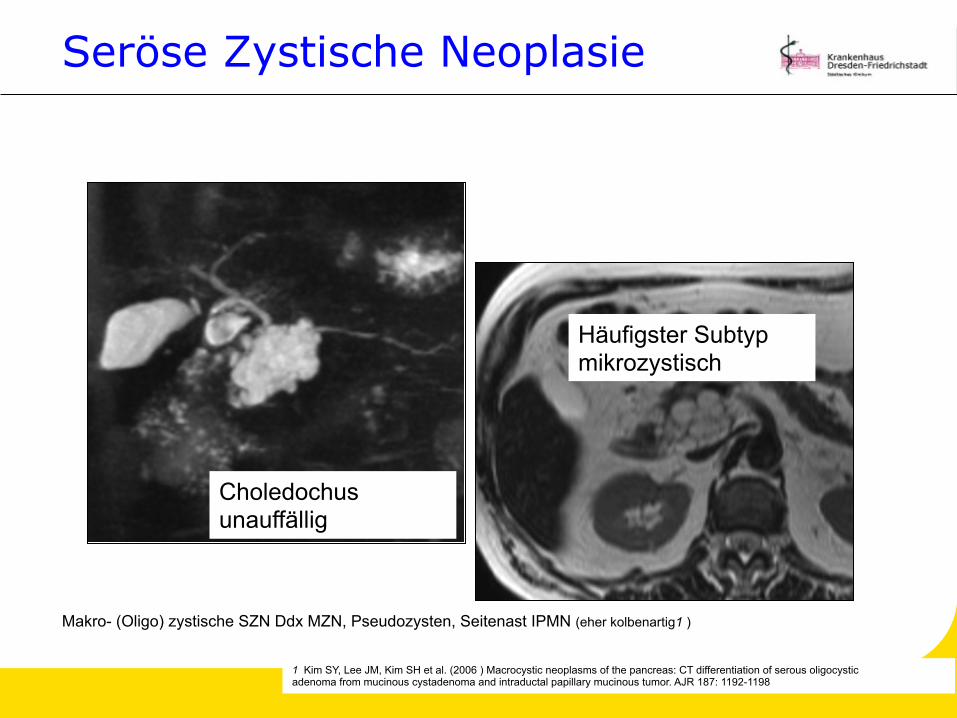
1 Kim SY, Lee JM, Kim SH et al. (2006 ) Macrocystic neoplasms of the pancreas: CT differentiation of serous oligocystic adenoma from mucinous cystadenoma and intraductal papillary mucinous tumor. AJR 187: 1192-1198
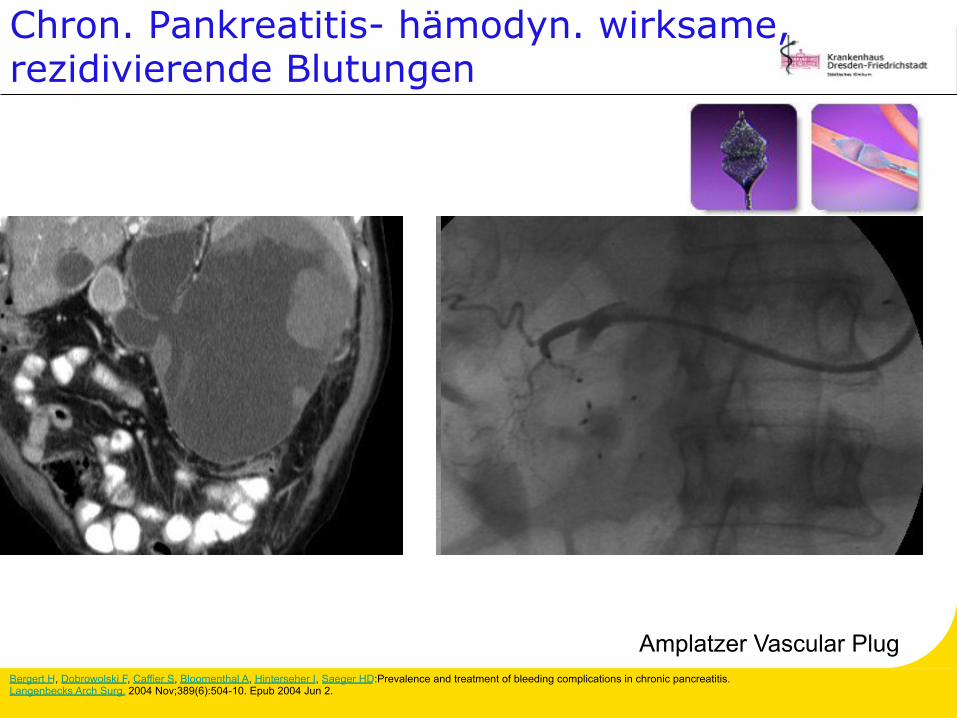
Bergert H, Dobrowolski F, Caffier S, Bloomenthal A, Hinterseher I, Saeger HD:Prevalence and treatment of bleeding complications in chronic pancreatitis. Langenbecks Arch Surg. 2004 Nov;389(6):504-10. Epub 2004 Jun 2.
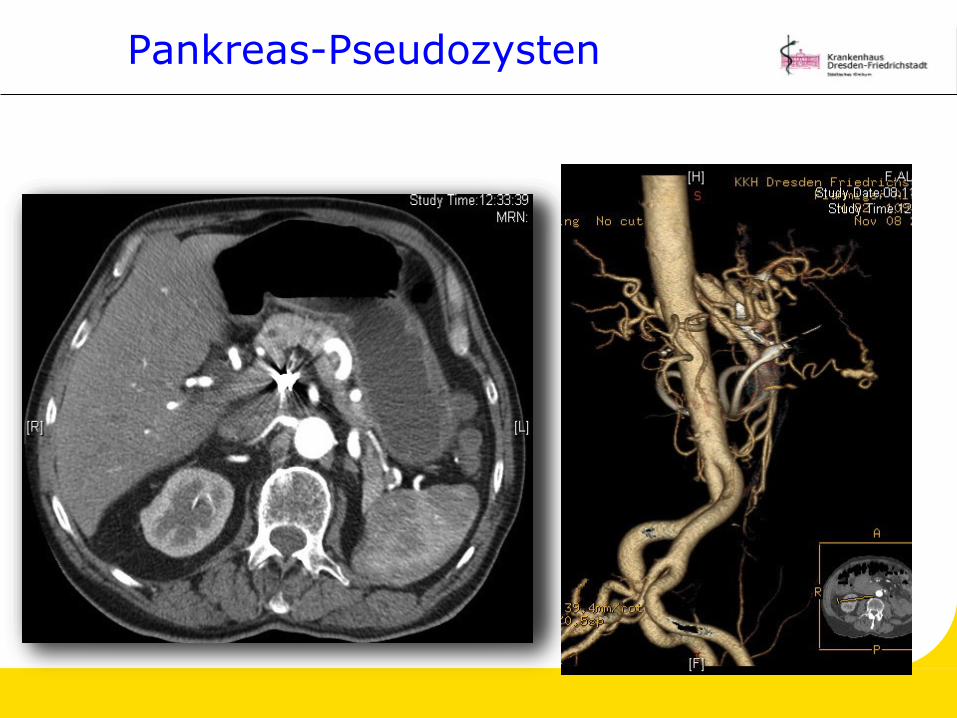
Pankreas-Pseudozysten
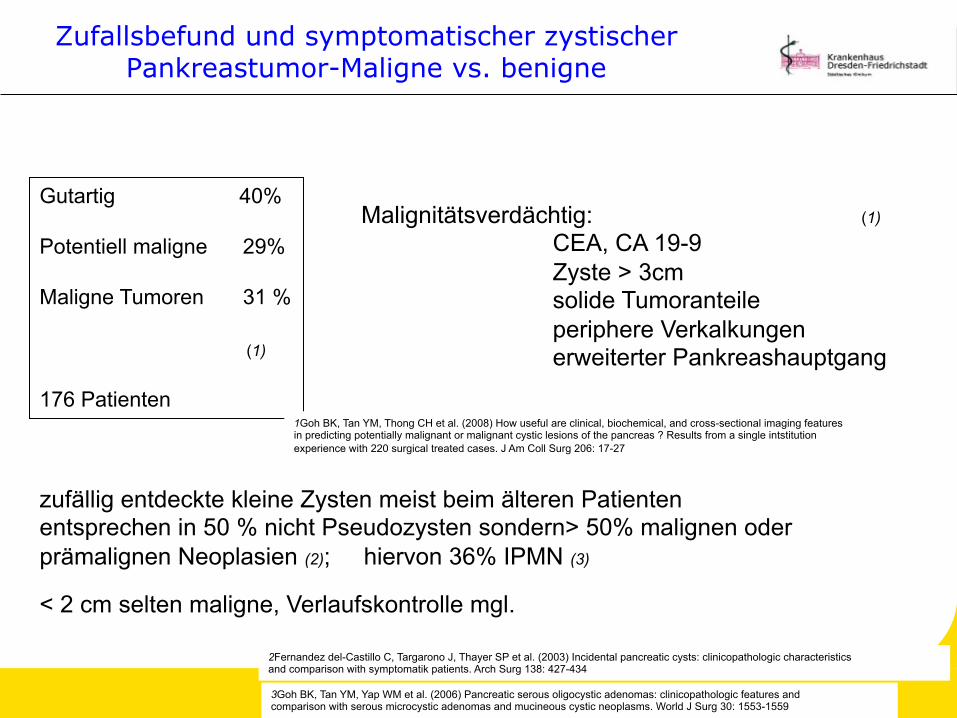
Zufallsbefund und symptomatischer zystischer Pankreastumor-Maligne vs. benigne
1Goh BK, Tan YM, Thong CH et al. (2008) How useful are clinical, biochemical, and cross-sectional imaging features in predicting potentially malignant or malignant cystic lesions of the pancreas ? Results from a single intstitution experience with 220 surgical treated cases. J Am Coll Surg 206: 17-27
zufällig entdeckte kleine Zysten meist beim älteren Patienten entsprechen in 50 % nicht Pseudozysten sondern> 50% malignen oder prämalignen Neoplasien (2); hiervon 36% IPMN (3)
< 2 cm selten maligne, Verlaufskontrolle mgl.
2Fernandez del-Castillo C, Targarono J, Thayer SP et al. (2003) Incidental pancreatic cysts: clinicopathologic characteristics and comparison with symptomatik patients. Arch Surg 138: 427-434
3Goh BK, Tan YM, Yap WM et al. (2006) Pancreatic serous oligocystic adenomas: clinicopathologic features and comparison with serous microcystic adenomas and mucineous cystic neoplasms. World J Surg 30: 1553-1559
S3-Leitlinie „Exokrines Pankreaskarzinom“ 2007 Ergebnis einer evidenzbasierten
Konsensukonferenz (13.-14.10.2006)
Bildgebende Verfahren zur Primär-Diagnostik
„Zur Klärung eines Tumorverdachts sind unterschiedliche Verfahren geeignet, wie Sonografie, Endosonografie, Multidetektor-CT, MRT mit MRCP oder ERCP“. Empfehlungsgrad B, Evidenzstärke 2, Konsens
Empfehlung „Diagnostische Verfahren der ersten Wahl zur Detektion des Pankreaskarzinoms sind die Oberbauchsonografie, die Endosonografie, die Multidetektor-CT-Untersuchung sowie die MRT in Kombination mit der MRCP.“ Empfehlungsgrad: B, Evidenzstärke 3, Konsens
Adler G, Seufferlein T, Bischoff SC et al. S3-Leitlinie „Exokrines Pankreaskarzinom“ Z Gastroenterol 2007; 45: 487-523
S3-Leitlinie „Exokrines Pankreaskarzinom“ 2007 Ergebnis einer evidenzbasierten
Konsensukonferenz (13.-14.10.2006)
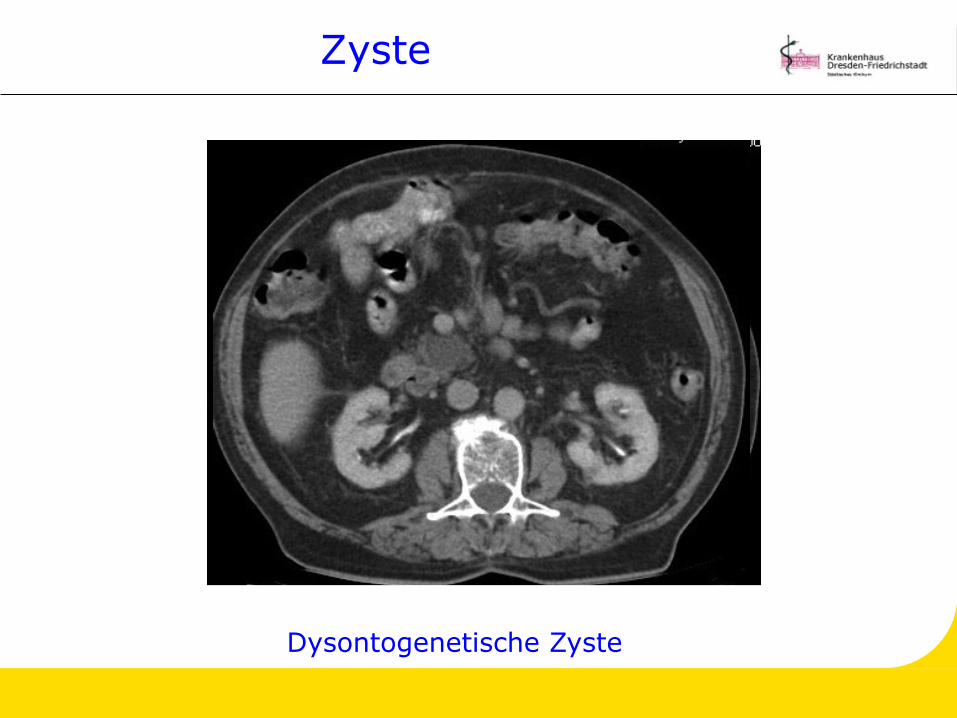
Zystische Prozesse
„Zur Differenzialdiagnostik zystischer Prozesse werden prinzipiell Oberbauchsonografie, die Multidetektor-CT-Untersuchung die MRT mit MRCP sowie die Endosonografie und die ERCP angewandt“. Empfehlungsgrad D, Evidenzstärke 3, Konsens
Anmerkungen „Keine der aufgeführten Methoden erlaubt eine eindeutige Diagnose. Allenfalls in Kombination mit den u.g. Verfahren (endosonografische Punktion mit CEA und CA 19-9 Bestimmung) lässt sich in Verbindung mit der jeweiligen klinischen Konstellation eine belastbare Aussage machen.“
Adler G, Seufferlein T, Bischoff SC et al. S3-Leitlinie „Exokrines Pankreaskarzinom“ Z Gastroenterol 2007; 45: 487-523
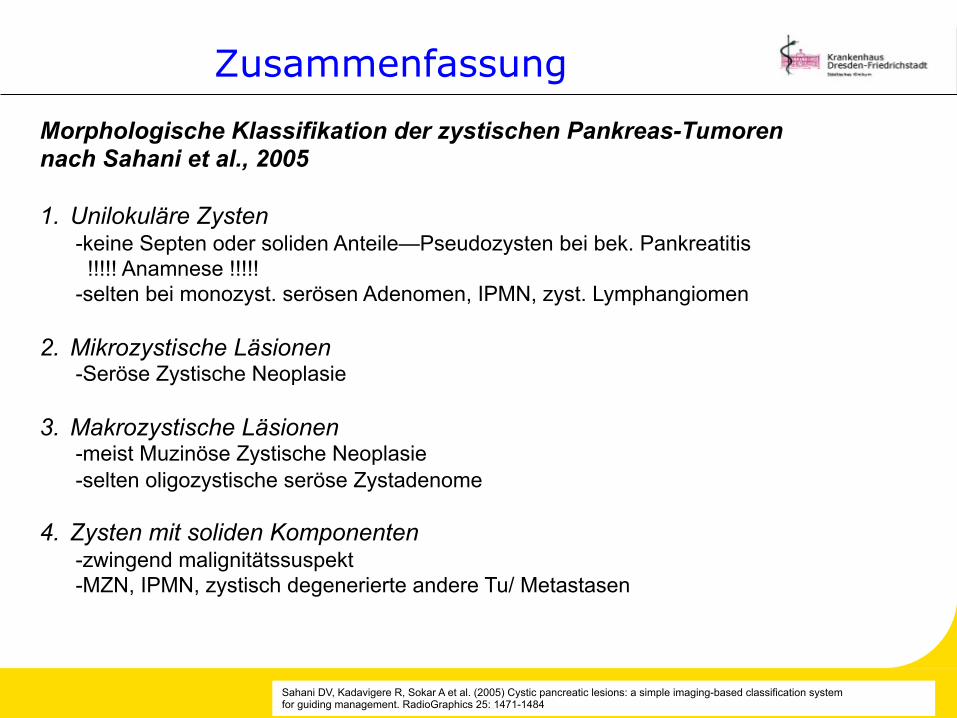
Sahani DV, Kadavigere R, Sokar A et al. (2005) Cystic pancreatic lesions: a simple imaging-based classification system for guiding management. RadioGraphics 25: 1471-1484
Morphologische Klassifikation der zystischen Pankreas-Tumoren nach Sahani et al., 2005 1. Unilokuläre Zysten
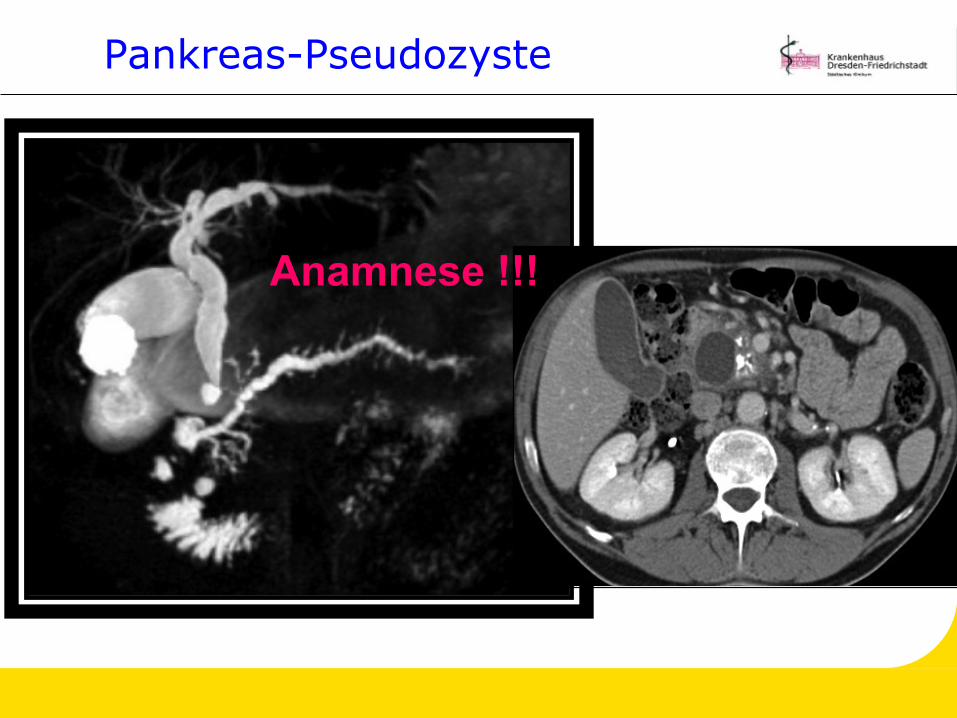
-keine Septen oder soliden Anteile—Pseudozysten bei bek. Pankreatitis !!!!! Anamnese !!!!! -selten bei monozyst. serösen Adenomen, IPMN, zyst. Lymphangiomen
4. Zysten mit soliden Komponenten -zwingend malignitätssuspekt -MZN, IPMN, zystisch degenerierte andere Tu/ Metastasen
Zusammenfassung
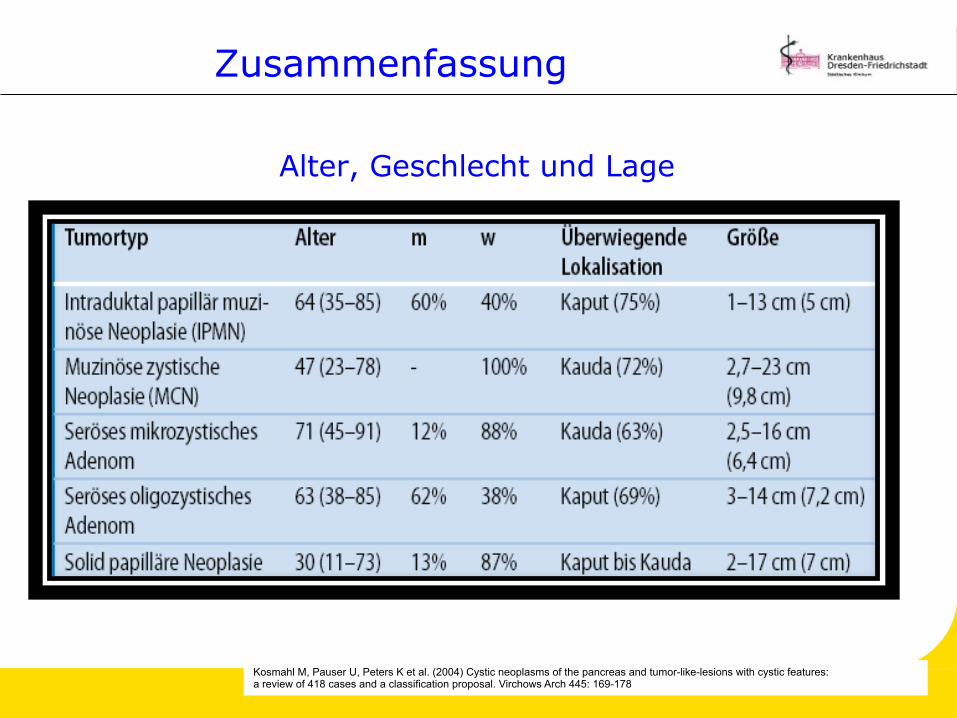
Alter, Geschlecht und Lage
Kosmahl M, Pauser U, Peters K et al. (2004) Cystic neoplasms of the pancreas and tumor-like-lesions with cystic features: a review of 418 cases and a classification proposal. Virchows Arch 445: 169-178
Zusammenfassung
Sahani DV, Saokar A, Hahn PF (2006) Pancreatic cysts 3 cm or smaller: how agressive should treatment be ? Radiology 238: 912-919
Morphologische Kriterien für maligne: (86 Patienten mit zufällig zystischen Tu < 3 cm):
Septierungen
Intrazystische, solide Vegetationen
Unilokulär und klein selten maligne (PPV 97%)
Zufallsbefund und symptomatischer zystischer Pankreastumor-Maligne vs. benigne
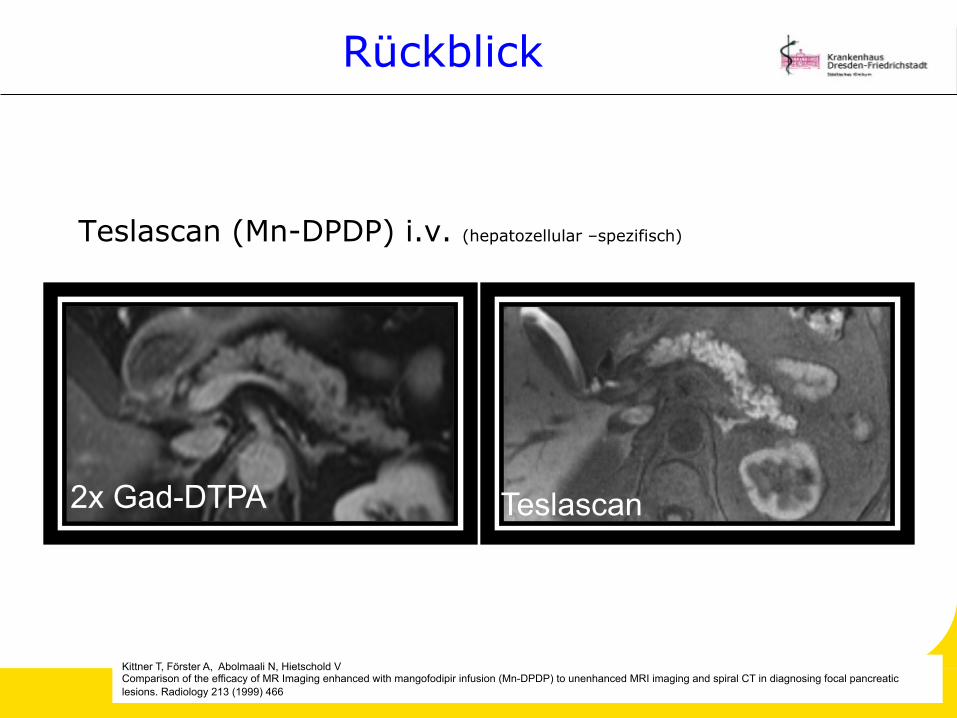
Kittner T, Förster A, Abolmaali N, Hietschold V Comparison of the efficacy of MR Imaging enhanced with mangofodipir infusion (Mn-DPDP) to unenhanced MRI imaging and spiral CT in diagnosing focal pancreatic lesions. Radiology 213 (1999) 466
2x Gad-DTPA Teslascan
Ausblick
Molekulare Bildgebung
MRT/ MR-Spektroskopie
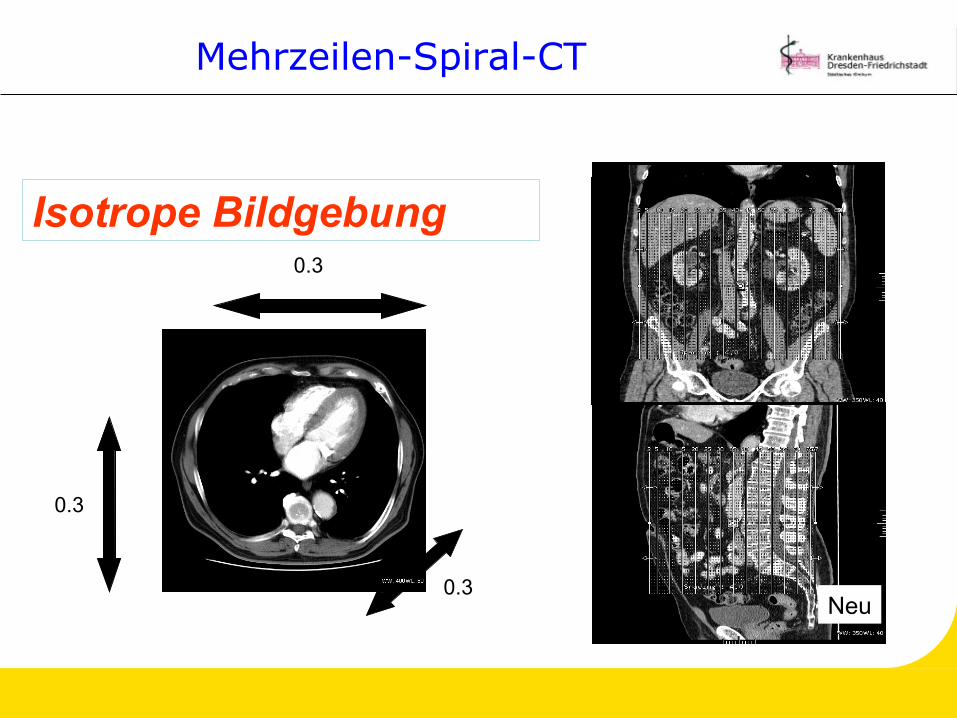
Mehrzeilen-Spiral-CT
Angiografie
Ultraschall
Röntgen
Anatomie
PET/ PET-CT/PET-MRT
Tumor-Biologie
Morphologie
Metabolismus
Vaskularisation/ Perfusion
Rezeptoren/ Gen-Expression
„ The features are
becoming clearer“
Klöppel G, Kosmahl M (2001) Cystic lesions and neoplasms of the pancreas. Pancreatology 1: 648-655
Panta rhei- alles fließt
„Alles fließt und nichts bleibt; es gibt nur ein ewiges Werden und Wandeln“












![Dok1 - MINIMAL INVASIV CENTER · cysticum colli congenitum bezeichnet. Weniger häufig Sind Manifestationen an Lippe Oder Zunge [2, 3] Vom Dünn- Oder Dickdarm ausgehende zystische](https://static.unterlagen.site/doc/80x56/5dd07b42d6be591ccb61324a/dok1-minimal-invasiv-cysticum-colli-congenitum-bezeichnet-weniger-hufig-sind.jpg)
![Tumorlehre I Basiswissen [Kompatibilitätsmodus] · •Plattenepithelkarzinom • verhornend • nicht verhornend • verrukös • papillomatös • Adenokarzinome • muzinöse](https://static.unterlagen.site/doc/80x56/5ba09ce109d3f2df578d2cc1/tumorlehre-i-basiswissen-kompatibilitaetsmodus-plattenepithelkarzinom-.jpg)






