27
Die Primärtherapie von Patienten mit Multiplem Myelom Martin Kropff Medizinische Klinik A, Universitätsklinikum Münster [email protected] [email protected]

Die Primärtherapie von Patienten mitMultiplem Myelom
Martin KropffMedizinische Klinik A, Universitätsklinikum Münster
[email protected]@web.de

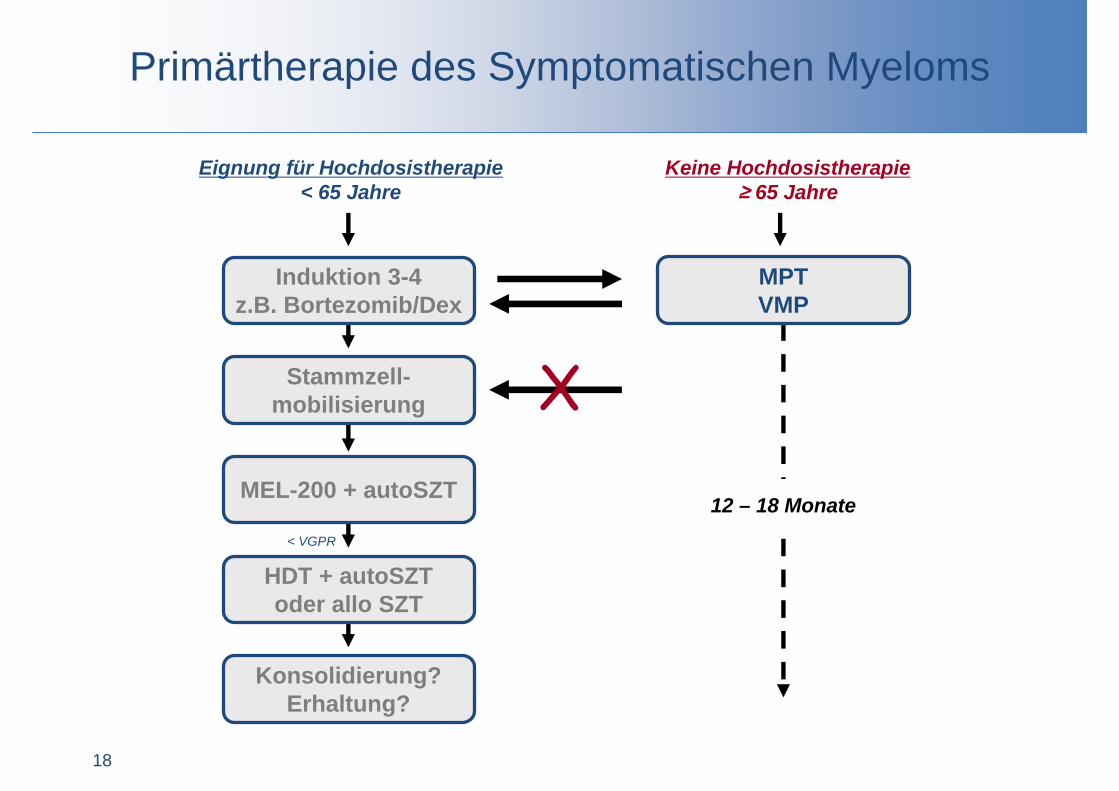
Primärtherapie des Symptomatischen Myeloms
2
Eignung für Hochdosistherapie< 65 Jahre
Keine Hochdosistherapie≥ 65 Jahre
Stammzell-mobilisierung
MEL-200 + autoSZT
HDT + autoSZToder allo SZT
12 – 18 Monate
Induktion 3-4z.B. Bortezomib/Dex
< VGPR
Konsolidierung?Erhaltung?
MPTVMP
X
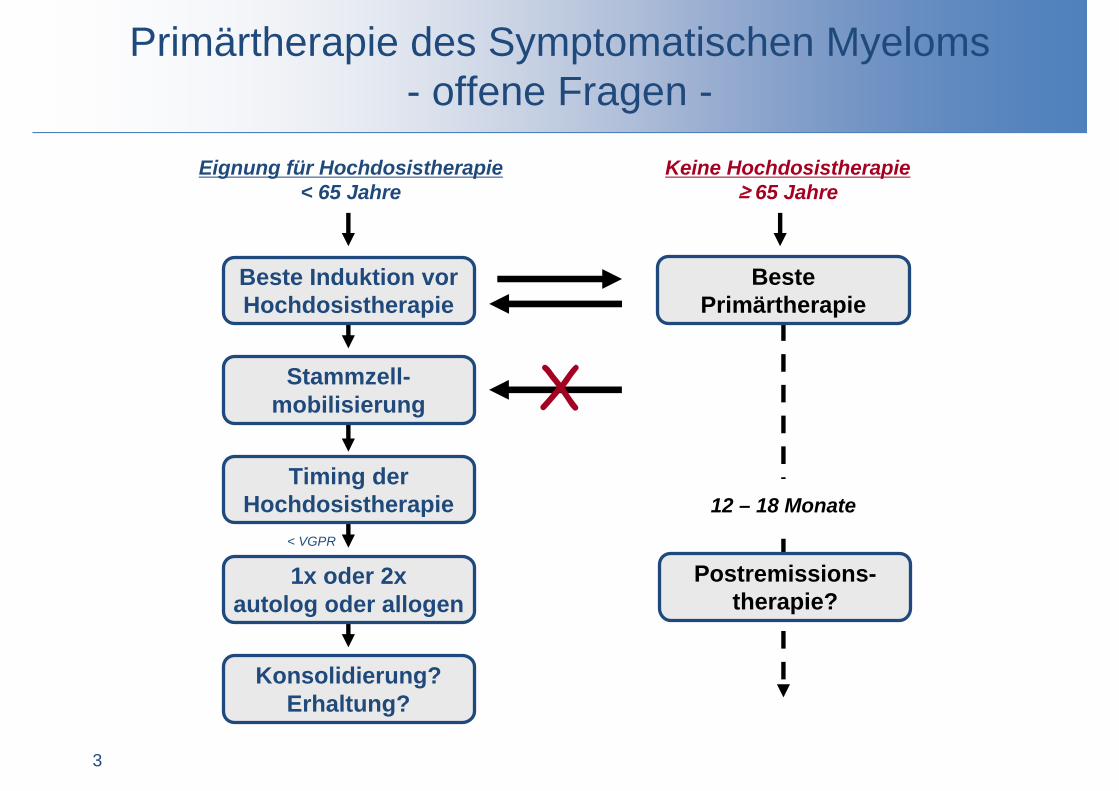
Primärtherapie des Symptomatischen Myeloms- offene Fragen -
3
Eignung für Hochdosistherapie< 65 Jahre
Keine Hochdosistherapie≥ 65 Jahre
Stammzell-mobilisierung
Timing der Hochdosistherapie
1x oder 2xautolog oder allogen
12 – 18 Monate
Beste Induktion vor Hochdosistherapie
< VGPR
Konsolidierung?Erhaltung?
Beste Primärtherapie
X
Postremissions-therapie?

Phase III-Studien zu Proteasom-Inhibitor- oder IMiD-basiertenInduktionen vor Hochdosistherapie bei MM
Regimen Phase N ORR(%)
CR(%)
Bortezomib/Dex[1-3] III 441 82 6
VTD[4] III 474 93 31(CR + nCR)
PAD[5] III 371 78 11Thal/Dex[6] III 204 63 4
Len/Dex[7,8]
(E4A03) III 445 81 13
Len/Dex[9]
(S0232) III 192 78 26
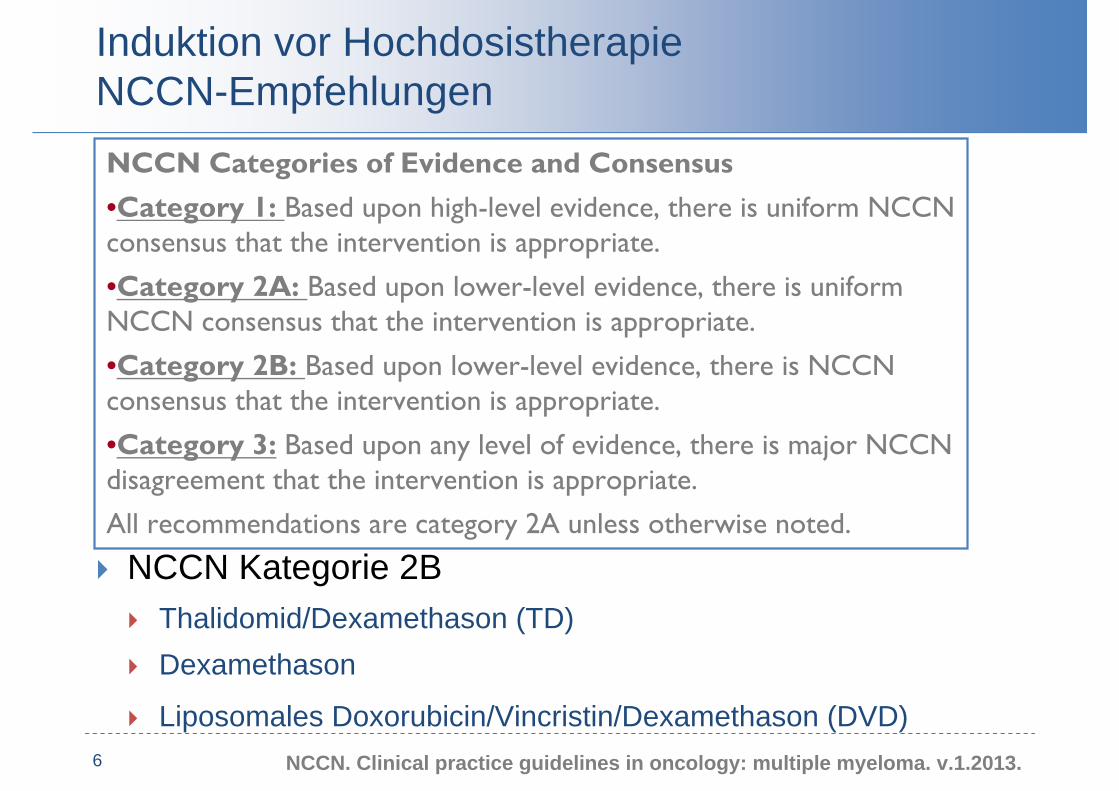
Induktion vor HochdosistherapieNCCN-Empfehlungen
6
NCCN Kategorie 1 Bortezomib/Dexamethason (VD) Bortezomib/Thalidomid/Dexamethason (VTD) Bortezomib/Doxorubicin/Dexamethason (PAD) Lenalidomid/Dexamethason (RD)
NCCN Kategorie 2A Bortezomib/Cyclophosphamid/Dexamethason (CyBorD) Bortezomib/Lenalidomid/Dexamethason (VRD)
NCCN Kategorie 2B Thalidomid/Dexamethason (TD) Dexamethason
Liposomales Doxorubicin/Vincristin/Dexamethason (DVD)NCCN. Clinical practice guidelines in oncology: multiple myeloma. v.1.2013.
NCCN Categories of Evidence and Consensus•Category 1: Based upon high-level evidence, there is uniform NCCN consensus that the intervention is appropriate.
•Category 2A: Based upon lower-level evidence, there is uniform NCCN consensus that the intervention is appropriate.
•Category 2B: Based upon lower-level evidence, there is NCCN consensus that the intervention is appropriate.
•Category 3: Based upon any level of evidence, there is major NCCN disagreement that the intervention is appropriate.
All recommendations are category 2A unless otherwise noted.

Suggested Approach to the Treatment of Newly Diagnosed Multiple Myeloma
•Palumbo A, Anderson K. N Engl J Med 2011;364:1046-1060

Risikostratifikation der Mayo-Clinic
Intermediäres Risiko*Standard Risiko Hohes Risiko*
BortezomibbedeutsamBortezomibbedeutsam
Erreichen einer CR
entscheidend
Erreichen einer CR
entscheidend
Günstiger Verlauf mit
jeder Therapie
Günstiger Verlauf mit
jeder Therapie
*Trisomien schwächen Risiko ab
• Hyperdiploid• t (11;14)• t (6;14)
• t (4;14) • del 17p• t (14;16)• t (14;20)• GEP definiertes
hohes Risiko
Prognose vergleichbar Standardrisiko bei Behandlung mit Bortezomib
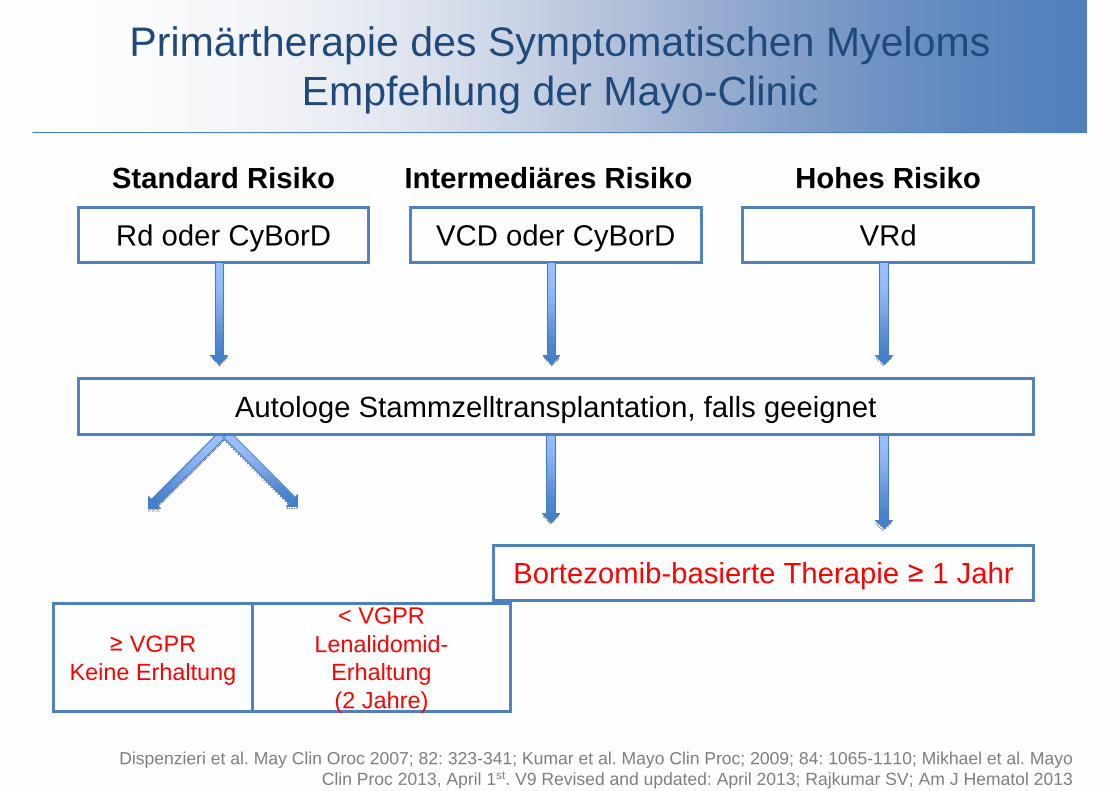
Primärtherapie des Symptomatischen MyelomsEmpfehlung der Mayo-Clinic
Intermediäres RisikoStandard Risiko Hohes Risiko
Rd oder CyBorD VCD oder CyBorD VRd
Autologe Stammzelltransplantation, falls geeignet
Bortezomib-basierte Therapie ≥ 1 Jahr< VGPR
Lenalidomid-Erhaltung(2 Jahre)
≥ VGPRKeine Erhaltung
Dispenzieri et al. May Clin Oroc 2007; 82: 323-341; Kumar et al. Mayo Clin Proc; 2009; 84: 1065-1110; Mikhael et al. Mayo Clin Proc 2013, April 1st. V9 Revised and updated: April 2013; Rajkumar SV; Am J Hematol 2013

15 30 45 60
25
50
75
100
Übe
rlebe
n (%
)
00
Hochdosis
Konventionelle Dosis
Monate20 40 60 80
25
50
75
100
Übe
rlebe
n (%
)
00
HochdosisMedianes OS: 54 Mo.
StandardtherapieMedianes OS: 42 Mo.
Monate
P = ,03 by Wilcoxon testP = ,04 by log rank test
Attal M, et al. N Engl J Med. 1996;335:91-97. Child JA, et al. N Engl J Med. 2003;348:1875-1883.
Hochdosistherapie und Stammzelltransplantation versus konventionell dosierte Therapie

Primärtherapie mit HochdosistherapieZeitpunkt der Dosisintensivierung
11
Stellenwert der Hochdosistherapie Stellenwert der Hochdosistherapie:
Metaanalyse 9 randomisierter Studien belegt eine längere Erkrankungskontrolle (PFS) verglichen mit einer konventionell dosierten Therapie.
Zeitpunkt der Hochdosistherapie:3 randomisierte Studien zeigen eine vergleichbares Überleben,
unabhängig vom Zeitpunkt der Hochdosistherapie im Erkrankungsverlauf.
Dosireduzierte Hochdosistherapie bei älteren Patienten?MP vs MPT vs Mel 100): Vorteil für MPT
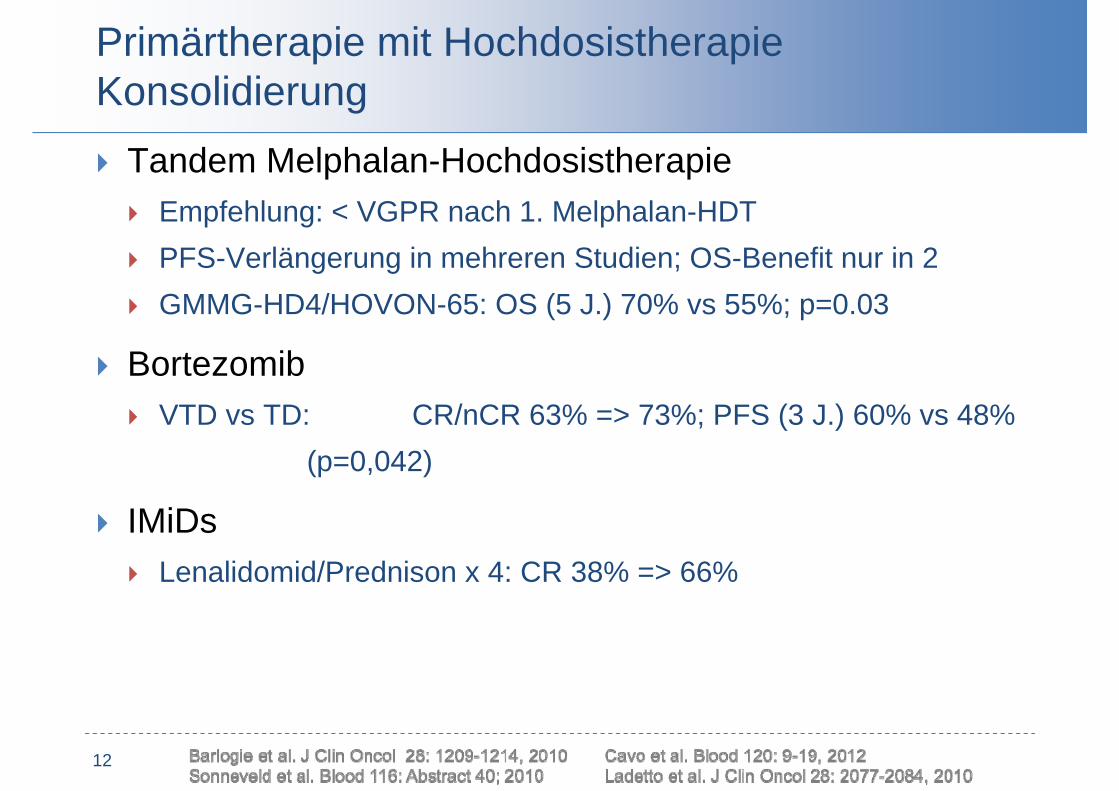
Primärtherapie mit HochdosistherapieKonsolidierung
12
Tandem Melphalan-Hochdosistherapie Empfehlung: < VGPR nach 1. Melphalan-HDT PFS-Verlängerung in mehreren Studien; OS-Benefit nur in 2 GMMG-HD4/HOVON-65: OS (5 J.) 70% vs 55%; p=0.03
Bortezomib VTD vs TD: CR/nCR 63% => 73%; PFS (3 J.) 60% vs 48%
(p=0,042)
IMiDs Lenalidomid/Prednison x 4: CR 38% => 66%

13 Cavo et al. ASH 2010 (Abstract 42)
• Thalidomid
• Lenalidomid
• Bortezomib
• +/- Prednison
• +/- Bisphosphonat
Primärtherapie mit HochdosistherapieErhaltung

Erhaltungstherapie mit Thalidomid
Trial N Erhaltung EFS oder PFS OSIFM 99-02[1] 597 Thalidomid + Pamidronat vs
Keine Erhaltung3-J. EFS: 52% vs 37%;
P < 0,009 4-yr OS: 87% vs 74%;
P < ,04
Spencer[2] 243 Thalidomid (12 Monate) + Prednison vs Prednison
3-J. PFS: 42% vs 23%; P < 0,001
3-yr OS: 86% vs 75%;P = ,004
Total Therapy 2[3] 668 Thalidomid vs keine Erhaltungbis zur Progression
5-J. EFS: 56% vs 45%; P = ,0005
5-yr OS: 67% vs 65%,8-yr OS: 57% vs 44%;
P = ,09
Lokhorst 2010[4] 556 Thalidomid vs IFN bis zur Progression
PFS: 34 vs 25 MonateP < ,001
73 vs 60 Monate; P = NS
Ludwig 2010[5] 289 Thalidomid + IFN vs IFN bis zur Progression
PFS: 27,7 vs 13,2 mos; P < 0,0068
52,6 vs 51,4 Monate;P = NS
MRC Myeloma IX[6] 820 Thalidomid vs keine Erhaltungbis zur Progression
PFS: 23 vs 15 Monate;
P < 0,000360 vs 58 Monate;
P = NS
NCIC CTG MY.10[7] 332 Thalidomid/Prednison vs keineErhaltung nach ASCT PFS: 28 vs 17 Monate
HOVON[8] 827 Bortezomib vs Thalidomid alsErhaltung nach PAD or VAD PFS: 28 vs 35 Monate
5-yr OS: 61% vs 55%
1. Attal M, et al. Blood. 2006;108:3289-3294. 2. Spencer A, et al. J Clin Oncol. 2009;27:1788-1793. 3. Barlogie B, et al. Blood. 2008;112:3115-3121. 4. Lokhorst HM, et al. Blood. 2010;115:1113-1120. 5. Ludwig H, et al. Haematologica. 2010;95:1548-1554. 6. Morgan GJ, et al. Blood. 2012;119:7-15. 7. Stewart AK, et al. ASH 2010. Abstract 39. 8. SonneveldP, et al. J Clin Oncol. 2012;30:2946-2955.
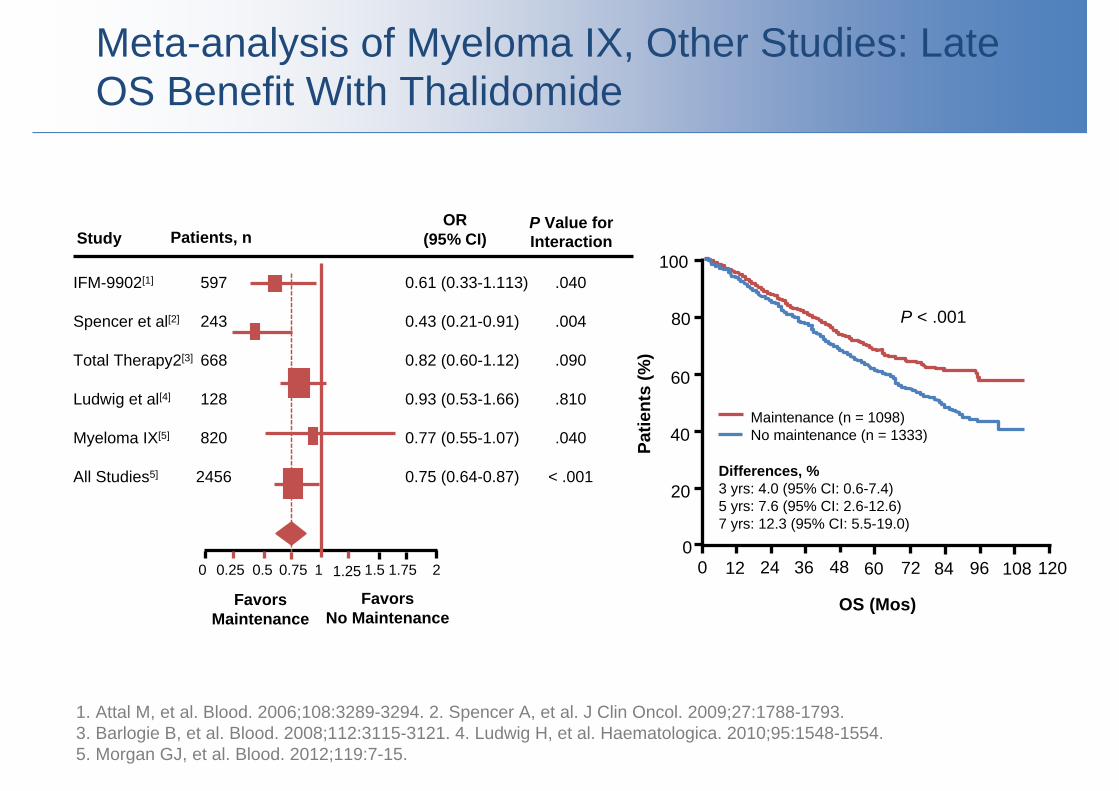
Meta-analysis of Myeloma IX, Other Studies: Late OS Benefit With Thalidomide
1. Attal M, et al. Blood. 2006;108:3289-3294. 2. Spencer A, et al. J Clin Oncol. 2009;27:1788-1793. 3. Barlogie B, et al. Blood. 2008;112:3115-3121. 4. Ludwig H, et al. Haematologica. 2010;95:1548-1554. 5. Morgan GJ, et al. Blood. 2012;119:7-15.
0 0.25 0.5 0.75 1 1.25 1.5 1.75 2
FavorsMaintenance
FavorsNo Maintenance
IFM-9902[1]
Spencer et al[2]
Total Therapy2[3]
Ludwig et al[4]
Myeloma IX[5]
All Studies5]
597
243
668
128
820
2456
Study Patients, nOR
(95% CI)P Value for Interaction
0.61 (0.33-1.113)
0.43 (0.21-0.91)
0.82 (0.60-1.12)
0.93 (0.53-1.66)
0.77 (0.55-1.07)
0.75 (0.64-0.87)
.040
.004
.090
.810
.040
< .001
100
80
60
40
20
0
Patie
nts
(%)
0 12 24 36 48 60 72
OS (Mos)
Maintenance (n = 1098)No maintenance (n = 1333)
84 96 108 120
P < .001
Differences, %3 yrs: 4.0 (95% CI: 0.6-7.4)5 yrs: 7.6 (95% CI: 2.6-12.6)7 yrs: 12.3 (95% CI: 5.5-19.0)

CALGB 100104: Lenalidomid vs Plazebo alsErhaltungstherapie nach autologer Transplantation
Ergebnis Lenalidomid(n = 231)
Placebo(n = 229)
P Wert HR(95% CI)
3-Jahres Progressionsfreiheit (%) 66 39 NR NR
3-Jahres Überleben (%) 88 80 NR 0.62(0.40-0.95)
McCarthy PL, et al. N Engl J Med. 2012;366:1770-1781.
0
20
40
60
80
100
0 10 30 45 50 60 70
PFS
(%)
Monate seit autologer Transplantation Monate seit autologer Transplantation
0
20
40
60
80
100
0 20 30 55 60 70
OS
(%)
401020
2-seitiges P < 0.001
Lenalidomid
Placebo
2-seitiges P = 0.03
Placebo
Lenalidomid
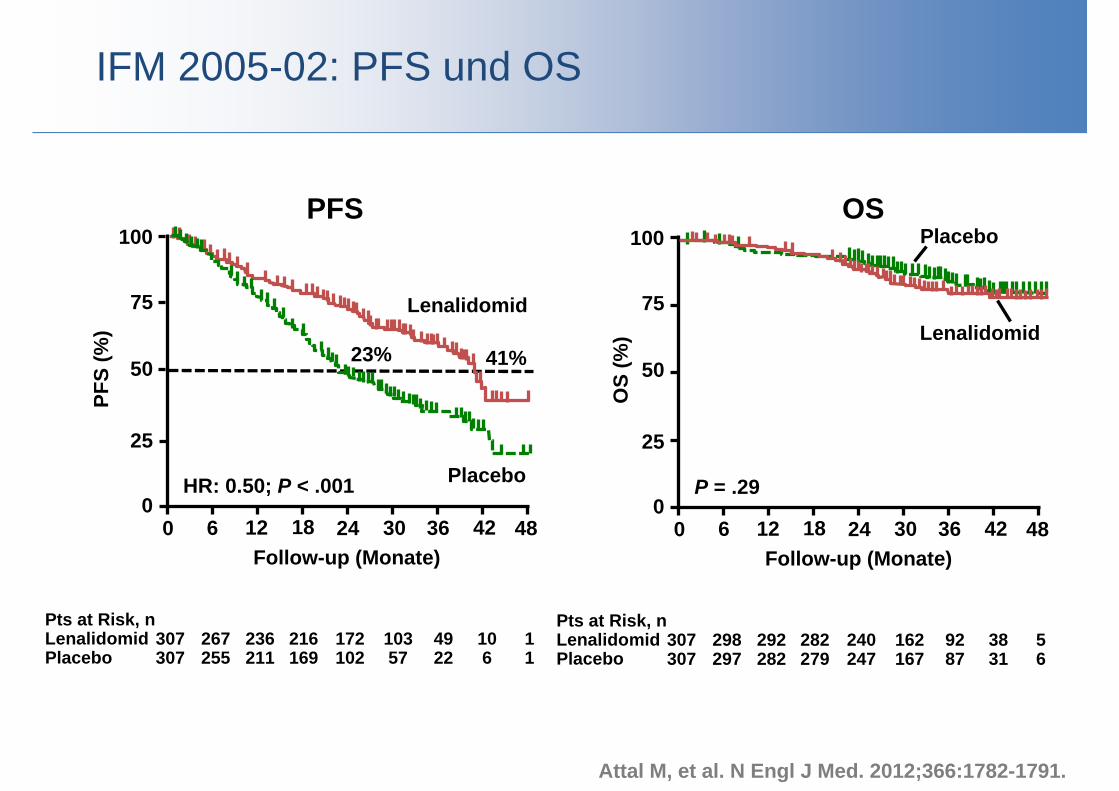
IFM 2005-02: PFS und OS
Attal M, et al. N Engl J Med. 2012;366:1782-1791.
PFS OS
HR: 0.50; P < .001
100
75
50
25
0
PFS
(%)
0 6 12 18 24 30 36 42 48Follow-up (Monate)
23% 41%
Lenalidomid
Placebo
Pts at Risk, nLenalidomidPlacebo
307307
267255
236211
216169
172102
10357
4922
106
11
P = .29
100
75
50
25
0
OS
(%)
0 6 12 18 24 30 36 42 48Follow-up (Monate)
Lenalidomid
Placebo
Pts at Risk, n LenalidomidPlacebo
307307
298297
292282
282279
240247
162167
9287
3831
56
Primärtherapie des Symptomatischen Myeloms
18
Eignung für Hochdosistherapie< 65 Jahre
Keine Hochdosistherapie≥ 65 Jahre
Stammzell-mobilisierung
MEL-200 + autoSZT
HDT + autoSZToder allo SZT
12 – 18 Monate
Induktion 3-4z.B. Bortezomib/Dex
< VGPR
Konsolidierung?Erhaltung?
MPTVMP
X
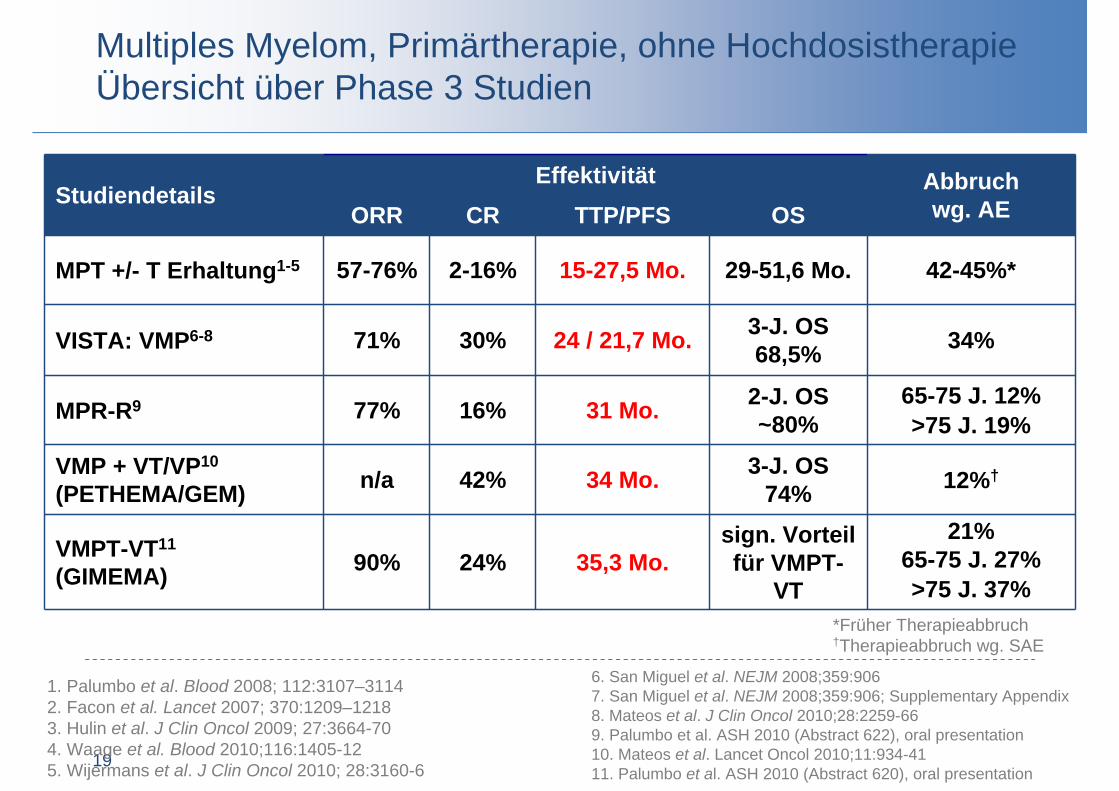
StudiendetailsEffektivität Abbruch
wg. AEORR CR TTP/PFS OS
MPT +/- T Erhaltung1-5 57-76% 2-16% 15-27,5 Mo. 29-51,6 Mo. 42-45%*
VISTA: VMP6-8 71% 30% 24 / 21,7 Mo. 3-J. OS68,5% 34%
MPR-R9 77% 16% 31 Mo. 2-J. OS~80%
65-75 J. 12%>75 J. 19%
VMP + VT/VP10
(PETHEMA/GEM) n/a 42% 34 Mo. 3-J. OS74% 12%†
VMPT-VT11
(GIMEMA) 90% 24% 35,3 Mo.sign. Vorteilfür VMPT-
VT
21%65-75 J. 27%>75 J. 37%
19
1. Palumbo et al. Blood 2008; 112:3107–31142. Facon et al. Lancet 2007; 370:1209–12183. Hulin et al. J Clin Oncol 2009; 27:3664-704. Waage et al. Blood 2010;116:1405-125. Wijermans et al. J Clin Oncol 2010; 28:3160-6
6. San Miguel et al. NEJM 2008;359:9067. San Miguel et al. NEJM 2008;359:906; Supplementary Appendix8. Mateos et al. J Clin Oncol 2010;28:2259-669. Palumbo et al. ASH 2010 (Abstract 622), oral presentation10. Mateos et al. Lancet Oncol 2010;11:934-4111. Palumbo et al. ASH 2010 (Abstract 620), oral presentation
*Früher Therapieabbruch†Therapieabbruch wg. SAE
Multiples Myelom, Primärtherapie, ohne HochdosistherapieÜbersicht über Phase 3 Studien
Palumbo A, Gringhen S, Rossi D, et al. Overall survival benefit for bortezomib-melphalan-prednisonethalidomide followed by maintenance with bortezomib-thalidomide (VMPT-VT) versus bortezomibmelphalan-prednisone (VMP) in newly diagnosed multiple myeloma patients. Program and abstracts of the 54th American Society of Hematology Annual Meeting and Exposition; December 8-11, 2012; Atlanta, Georgia. Abstract 200.Palumbo A, Bringhen S, Rossi D, et al. Bortezomib-melphalan-prednisone-thalidomide followed by maintenance with bortezomib-thalidomide compared with bortezomib-melphalan-prednisone for initial treatment of multiple myeloma: a randomized controlled trial. J Clin Oncol. 2010;28:5101-5109.
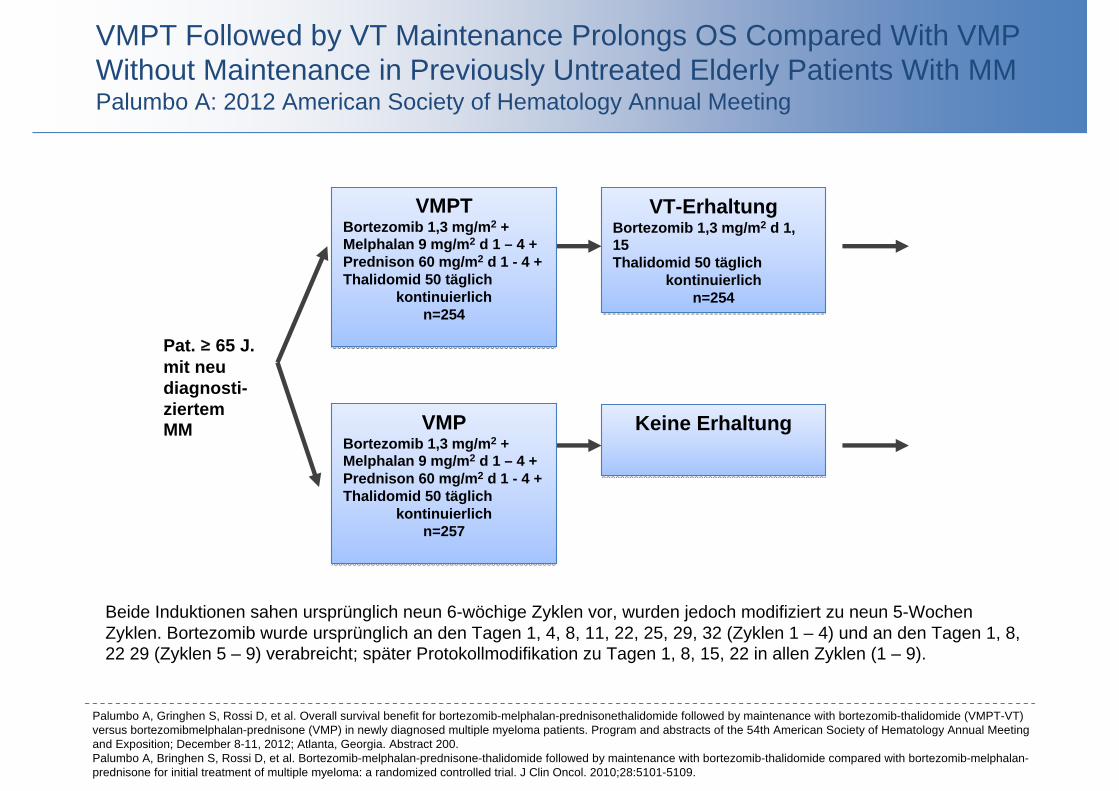
VMPT Followed by VT Maintenance Prolongs OS Compared With VMP Without Maintenance in Previously Untreated Elderly Patients With MMPalumbo A: 2012 American Society of Hematology Annual Meeting
VT-ErhaltungBortezomib 1,3 mg/m2 d 1, 15Thalidomid 50 täglich
kontinuierlichn=254
VT-ErhaltungBortezomib 1,3 mg/m2 d 1, 15Thalidomid 50 täglich
kontinuierlichn=254
VMPTBortezomib 1,3 mg/m2 + Melphalan 9 mg/m2 d 1 – 4 +Prednison 60 mg/m2 d 1 - 4 + Thalidomid 50 täglich
kontinuierlichn=254
VMPTBortezomib 1,3 mg/m2 + Melphalan 9 mg/m2 d 1 – 4 +Prednison 60 mg/m2 d 1 - 4 + Thalidomid 50 täglich
kontinuierlichn=254
VMPBortezomib 1,3 mg/m2 + Melphalan 9 mg/m2 d 1 – 4 +Prednison 60 mg/m2 d 1 - 4 + Thalidomid 50 täglich
kontinuierlichn=257
VMPBortezomib 1,3 mg/m2 + Melphalan 9 mg/m2 d 1 – 4 +Prednison 60 mg/m2 d 1 - 4 + Thalidomid 50 täglich
kontinuierlichn=257
Keine ErhaltungKeine Erhaltung
Pat. ≥ 65 J. mit neu diagnosti-ziertemMM
Beide Induktionen sahen ursprünglich neun 6-wöchige Zyklen vor, wurden jedoch modifiziert zu neun 5-Wochen Zyklen. Bortezomib wurde ursprünglich an den Tagen 1, 4, 8, 11, 22, 25, 29, 32 (Zyklen 1 – 4) und an den Tagen 1, 8, 22 29 (Zyklen 5 – 9) verabreicht; später Protokollmodifikation zu Tagen 1, 8, 15, 22 in allen Zyklen (1 – 9).
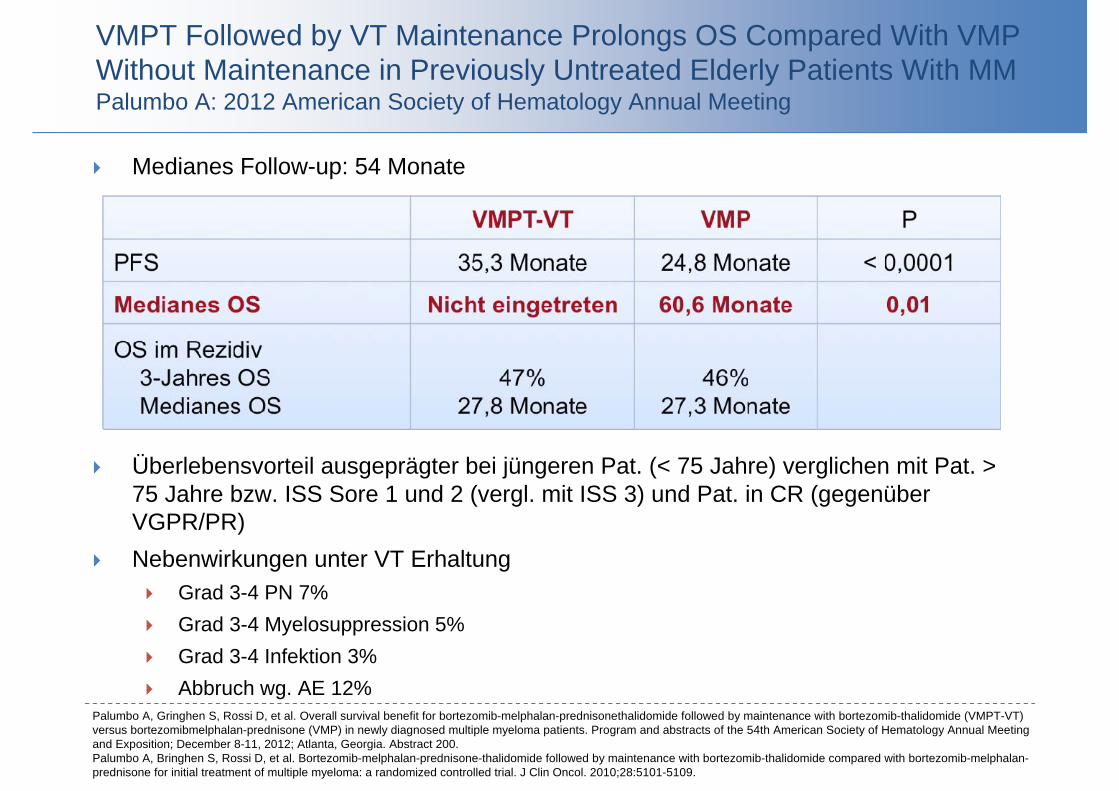
Medianes Follow-up: 54 Monate
Palumbo A, Gringhen S, Rossi D, et al. Overall survival benefit for bortezomib-melphalan-prednisonethalidomide followed by maintenance with bortezomib-thalidomide (VMPT-VT) versus bortezomibmelphalan-prednisone (VMP) in newly diagnosed multiple myeloma patients. Program and abstracts of the 54th American Society of Hematology Annual Meeting and Exposition; December 8-11, 2012; Atlanta, Georgia. Abstract 200.Palumbo A, Bringhen S, Rossi D, et al. Bortezomib-melphalan-prednisone-thalidomide followed by maintenance with bortezomib-thalidomide compared with bortezomib-melphalan-prednisone for initial treatment of multiple myeloma: a randomized controlled trial. J Clin Oncol. 2010;28:5101-5109.
VMPT Followed by VT Maintenance Prolongs OS Compared With VMP Without Maintenance in Previously Untreated Elderly Patients With MMPalumbo A: 2012 American Society of Hematology Annual Meeting
Überlebensvorteil ausgeprägter bei jüngeren Pat. (< 75 Jahre) verglichen mit Pat. > 75 Jahre bzw. ISS Sore 1 und 2 (vergl. mit ISS 3) und Pat. in CR (gegenüberVGPR/PR)
Nebenwirkungen unter VT Erhaltung Grad 3-4 PN 7% Grad 3-4 Myelosuppression 5% Grad 3-4 Infektion 3% Abbruch wg. AE 12%

Palumbo A, Gringhen S, Rossi D, et al. Overall survival benefit for bortezomib-melphalan-prednisonethalidomide followed by maintenance with bortezomib-thalidomide (VMPT-VT) versus bortezomibmelphalan-prednisone (VMP) in newly diagnosed multiple myeloma patients. Program and abstracts of the 54th American Society of Hematology Annual Meeting and Exposition; December 8-11, 2012; Atlanta, Georgia. Abstract 200.Palumbo A, Bringhen S, Rossi D, et al. Bortezomib-melphalan-prednisone-thalidomide followed by maintenance with bortezomib-thalidomide compared with bortezomib-melphalan-prednisone for initial treatment of multiple myeloma: a randomized controlled trial. J Clin Oncol. 2010;28:5101-5109.
VMPT Followed by VT Maintenance Prolongs OS Compared With VMP Without Maintenance in Previously Untreated Elderly Patients With MMPalumbo A: 2012 American Society of Hematology Annual Meeting
VMP VMPT-VT
0
0.25
0.50
0.75
1.00
0
Patie
nten
10 20 30 40 50 60 70 80
PFS42% reduziertes Progressionsrisiko
Median 35,3 Monate
Median 24,8 MonateHR: 0.58 (95% CI: 0.47-0.71; P < .0001)
Monate
0
0.25
0.50
0.75
1.00
0 10 20 30 40 50 60 70 80
TTNT48% reduziertes Risiko erneuten Therapy
Median 46,6 Monate
Median 27,8 MonateHR: 0.52 (95% CI: 0.42-0.66; P < .0001)
Monate

Palumbo A, Gringhen S, Rossi D, et al. Overall survival benefit for bortezomib-melphalan-prednisonethalidomide followed by maintenance with bortezomib-thalidomide (VMPT-VT) versus bortezomibmelphalan-prednisone (VMP) in newly diagnosed multiple myeloma patients. Program and abstracts of the 54th American Society of Hematology Annual Meeting and Exposition; December 8-11, 2012; Atlanta, Georgia. Abstract 200.Palumbo A, Bringhen S, Rossi D, et al. Bortezomib-melphalan-prednisone-thalidomide followed by maintenance with bortezomib-thalidomide compared with bortezomib-melphalan-prednisone for initial treatment of multiple myeloma: a randomized controlled trial. J Clin Oncol. 2010;28:5101-5109.
VMPT Followed by VT Maintenance Prolongs OS Compared With VMP Without Maintenance in Previously Untreated Elderly Patients With MMPalumbo A: 2012 American Society of Hematology Annual Meeting
Überleben
30% reduziertesTodesrisiko
Medianes Überleben nach Rezidiv und Start einer Rezidivtherapie unbeeinflusstvon Primärtherapie VMPT → VT und VMP Arme: 27,8 vs 27,3 Monate (HR: 0,92; 95% CI: 0,66-1,28; P = .63)
3-Jahres Überleben nach Rezidiv: 47% VMPT → VT vs 46% VMP
0
0.25
0.50
0.75
1.00
0
Patie
nten
10 20 30 40 50 60 70 90Monate
80
^therapy
HR: 0,70 (95% CI: 0,52-0,92; P = ,01)
5-J. OS, %6151
Medianes Überlebenn.e.
60,6 MonateVMPT-VTVMP
VMPT VT Maintenance

Palumbo A, Gringhen S, Rossi D, et al. Overall survival benefit for bortezomib-melphalan-prednisonethalidomide followed by maintenance with bortezomib-thalidomide (VMPT-VT) versus bortezomibmelphalan-prednisone (VMP) in newly diagnosed multiple myeloma patients. Program and abstracts of the 54th American Society of Hematology Annual Meeting and Exposition; December 8-11, 2012; Atlanta, Georgia. Abstract 200.Palumbo A, Bringhen S, Rossi D, et al. Bortezomib-melphalan-prednisone-thalidomide followed by maintenance with bortezomib-thalidomide compared with bortezomib-melphalan-prednisone for initial treatment of multiple myeloma: a randomized controlled trial. J Clin Oncol. 2010;28:5101-5109.
VMPT Followed by VT Maintenance Prolongs OS Compared With VMP Without Maintenance in Previously Untreated Elderly Patients With MMPalumbo A: 2012 American Society of Hematology Annual Meeting
Bei älteren Patienen mit MM ist VMPT-VT dem VMP überlegen PFS: 42% reduziertes Progressionsrisiko TTNT: 48% reduziertes Risiko einer erneuten Therapie OS: 30% reduziertes Risiko, zu versterben
OS nach Rezidivtherapie unbeeinflusst von Primärtherapie
Günstigerer Verlauf bei Pat. < 75 Jahre, ISS Stage I-II sowie bei Erreichen zumindest einer CR nach VMPT
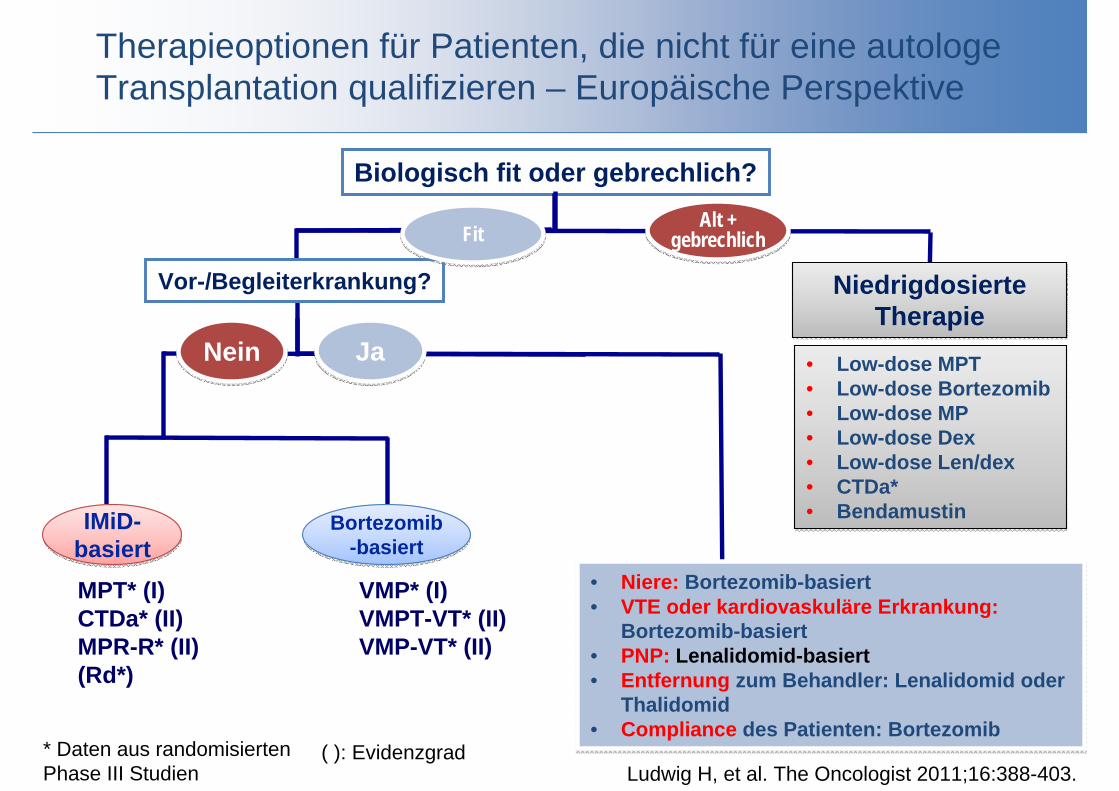
Therapieoptionen für Patienten, die nicht für eine autologe Transplantation qualifizieren – Europäische Perspektive
Biologisch fit oder gebrechlich?
• MPT* (I)• CTDa* (II)• MPR-R* (II)• (Rd*)
• VMP* (I)• VMPT-VT* (II)• VMP-VT* (II)
JaJa
IMiD-basiertIMiD-
basiertBortezomib
-basiertBortezomib
-basiert
Vor-/Begleiterkrankung?
* Daten aus randomisiertenPhase III Studien
( ): Evidenzgrad
• Niere: Bortezomib-basiert• VTE oder kardiovaskuläre Erkrankung:
Bortezomib-basiert• PNP: Lenalidomid-basiert• Entfernung zum Behandler: Lenalidomid oder
Thalidomid• Compliance des Patienten: Bortezomib
• Niere: Bortezomib-basiert• VTE oder kardiovaskuläre Erkrankung:
Bortezomib-basiert• PNP: Lenalidomid-basiert• Entfernung zum Behandler: Lenalidomid oder
Thalidomid• Compliance des Patienten: Bortezomib
NeinNein
Ludwig H, et al. The Oncologist 2011;16:388-403.
Alt + gebrechlich
Alt + gebrechlichFitFit
• Low-dose MPT• Low-dose Bortezomib• Low-dose MP• Low-dose Dex• Low-dose Len/dex• CTDa*• Bendamustin
• Low-dose MPT• Low-dose Bortezomib• Low-dose MP• Low-dose Dex• Low-dose Len/dex• CTDa*• Bendamustin
NiedrigdosierteTherapie
NiedrigdosierteTherapie

Sekundärmalignome
Studie Regime N Medianes PFS(Monate)
P Wert für PFS
3-J. OS Rate (%)
Medianes OS (Monate)
P Wert für OS
Sekundär-malignom(%)
P Wert für Sekundär-malignom
McCarthy2012
PlazeboLenalidomid
229231
2746 <0,001 80
88n.e.n.e. 0,03 2,6
7,7 0,008
Attal2012
PlazeboLenalidomid
307307
2341
<0,001 8480
n.e.n.e. 0,70 3,0
7,5 0,002
Palumbo2012
MPRMPRMP-R
154153152
131431
<0,001 666270
n.e.n.2.45
n,s.377
n.a.
n.e., nicht eingetreten bzw. nicht erreichtn.s., nicht signifikantn.a., nicht angegeben
Rajkumar SV, et al. Nat Rev Clin Oncol 2012
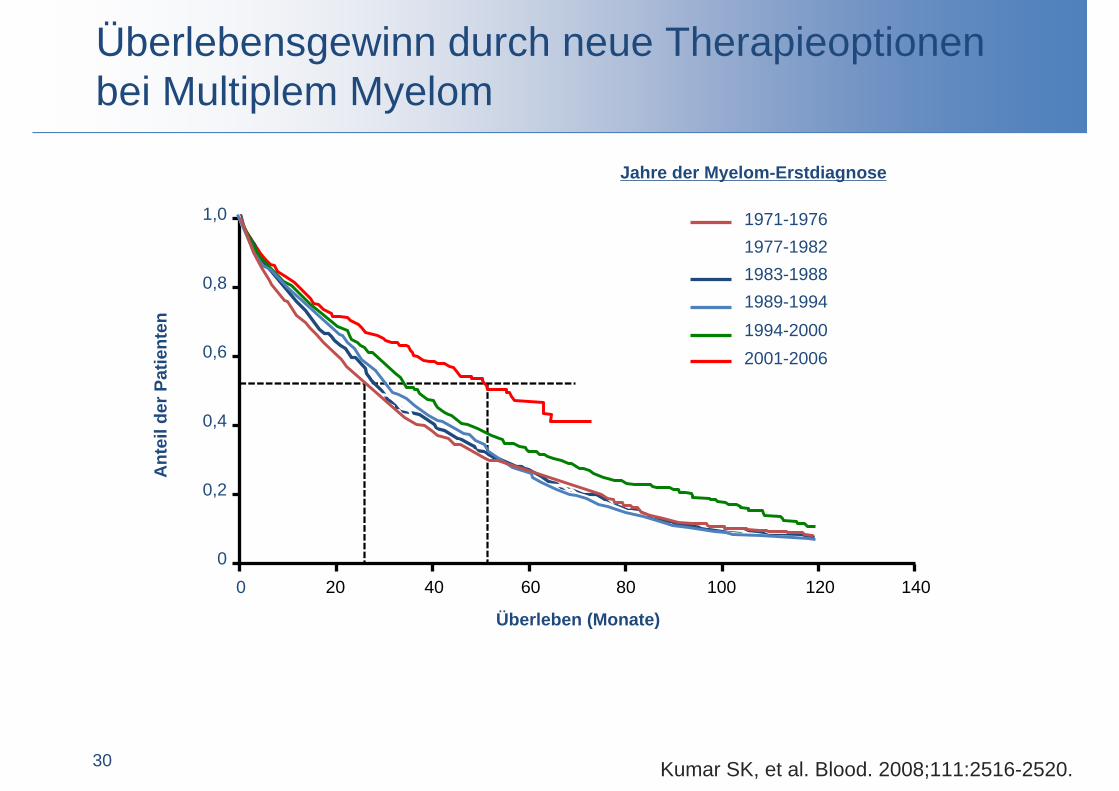
Überlebensgewinn durch neue Therapieoptionenbei Multiplem Myelom
30
Überleben (Monate)
Ant
eild
erPa
tient
en
0
0,2
0,4
0,6
0,8
1,0
0 20 40 60 80 100 120 140
1994-20002001-2006
1989-19941983-19881977-19821971-1976
Jahre der Myelom-Erstdiagnose
Kumar SK, et al. Blood. 2008;111:2516-2520.

State of the ArtDie Primärtherapie von Patienten mit Multiplem Myelom
32
Primärtherapie jüngerer Patienten Induktion mit Zweier-Kombinationen oder Triplets
Singuläre Melphalan-Hochdosistherapie
Konsolidierungen werden kommen
Erhaltung: Individualentscheidung (Thalidomid oder Lenalidomid)
Allogene Transplantatioon nur innerhalb klinischer Studien
Primärtherapie ältere Patienten MPT oder VMP
VMPT-VT besser als VMP allein 42% reduziertes Profressionsrisiko
30% reduzierte Sterblichkeit
Keine „Hochdosistherapie“ mit 100 mg/m2 Melphalan
Sekundäre primäre Malignome Thalidomid
Lenalidomid

















