Klinik für Anästhesiologie, Intensivmedizin und Schmerztherapie Direktor: Prof. Dr. Dr. Kai Zacharowski, FRCA Institut für Transfusionsmedizin und Immunhämatologie DRK-Blutspendedienst Baden-Württemberg – Hessen Direktor: Prof. Dr. Dr. Erhard Seifried Blutprodukte beim blutenden Patienten - Contra (=individuell) Patrick Meybohm Universitätsklinikum Frankfurt
Transcript
Corporate-Design-Farbe - orange (Goethe-Univ.): R = 237 G = 167 B = 45
Klinik für Anästhesiologie, Intensivmedizin und Schmerztherapie Direktor: Prof. Dr. Dr. Kai Zacharowski, FRCA
Institut für Transfusionsmedizin und Immunhämatologie DRK-Blutspendedienst Baden-Württemberg – Hessen Direktor: Prof. Dr. Dr. Erhard Seifried
Blutprodukte beim blutenden Patienten - Contra (=individuell)
Patrick Meybohm
Universitätsklinikum Frankfurt
Ergänzende Farbe grau: R = 100 G = 100 B = 100
Institut für Transfusionsmedizin und Immunhämatologie DRK-Blutspendedienst Baden-Württemberg – Hessen Direktor: Prof. Dr. Dr. Erhard Seifried
Klinik für Anästhesiologie, Intensivmedizin und Schmerztherapie Direktor: Prof. Dr. Dr. Kai Zacharowski, FRCA
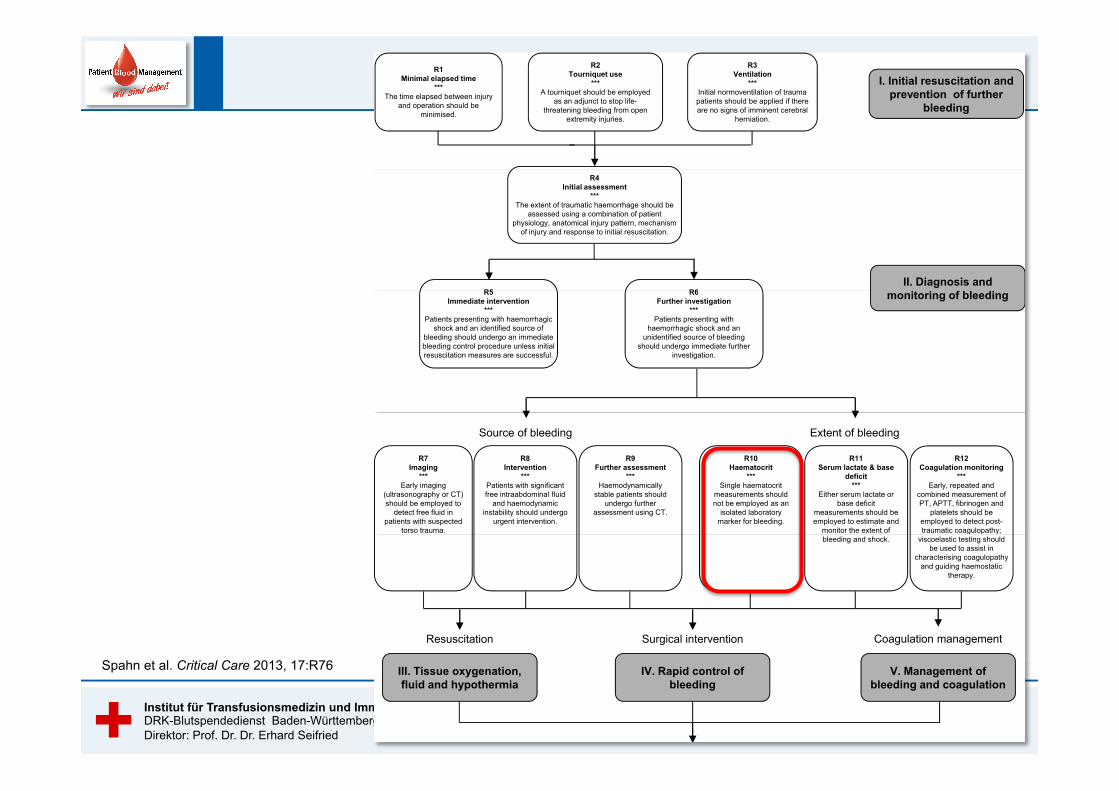
establishment of a European trauma database that includespre-defined quality indicators such as the time required tostop bleeding, 30-day mortality and morbidity. The newlyinitiated campaign aims to support institutions in the
development and implementation of locally adapted proto-cols, assist in the definition of management bundles andencourage each institution to establish systems with whichto assess compliance with the management strategy.
I. Initial resuscitation and prevention of further
bleeding
R3Ventilation
***Initial normoventilation of trauma patients should be applied if there are no signs of imminent cerebral
herniation.
R1Minimal elapsed time
***The time elapsed between injury
and operation should be minimised.
R2Tourniquet use
***A tourniquet should be employed
as an adjunct to stop life-threatening bleeding from open
extremity injuries.
R6II. Diagnosis and
f
R4Initial assessment
***The extent of traumatic haemorrhage should be
assessed using a combination of patient physiology, anatomical injury pattern, mechanism
of injury and response to initial resuscitation.
R5 R6Further investigation
***Patients presenting with
haemorrhagic shock and an unidentified source of bleeding
should undergo immediate further investigation.
monitoring of bleedingR5Immediate intervention
***Patients presenting with haemorrhagic
shock and an identified source of bleeding should undergo an immediate bleeding control procedure unless initial resuscitation measures are successful.
Extent of bleeding
R11Serum lactate & base
deficit***
Either serum lactate or base deficit
measurements should be employed to estimate and
monitor the extent of
R9Further assessment
***Haemodynamically
stable patients should undergo further
assessment using CT.
Source of bleeding
R8Intervention
***Patients with significant free intraabdominal fluid
and haemodynamicinstability should undergo
urgent intervention.
R7Imaging
***Early imaging
(ultrasonography or CT) should be employed to
detect free fluid in patients with suspected
torso trauma.
R10Haematocrit
***Single haematocrit
measurements should not be employed as an
isolated laboratory marker for bleeding.
R12Coagulation monitoring
***Early, repeated and
combined measurement of PT, APTT, fibrinogen and
platelets should be employed to detect post-traumatic coagulopathy;
implement an evidence-based treatment algorithm for the
bleeding trauma patient.
R36Checklists
***Treatment checklists
should be used to guide clinical management.
R37Quality management
***Each institution should include an assessment
of adherence to the institutional algorithm in
routine quality management
Figure 2 Flow chart of treatment modalities for the bleeding trauma patient discussed in this guideline (Part 1 of 2). APTT, activatedpartial thromboplastin time; CT, computed tomography; Hb, haemoglobin; PCC, prothrombin complex concentrate; PT, prothrombin time.
Spahn et al. Critical Care 2013, 17:R76http://ccforum.com/content/17/2/R76
Page 29 of 45
Spahn et al. Critical Care 2013, 17:R76
Ergänzende Farbe grau: R = 100 G = 100 B = 100
Institut für Transfusionsmedizin und Immunhämatologie DRK-Blutspendedienst Baden-Württemberg – Hessen Direktor: Prof. Dr. Dr. Erhard Seifried
Klinik für Anästhesiologie, Intensivmedizin und Schmerztherapie Direktor: Prof. Dr. Dr. Kai Zacharowski, FRCA
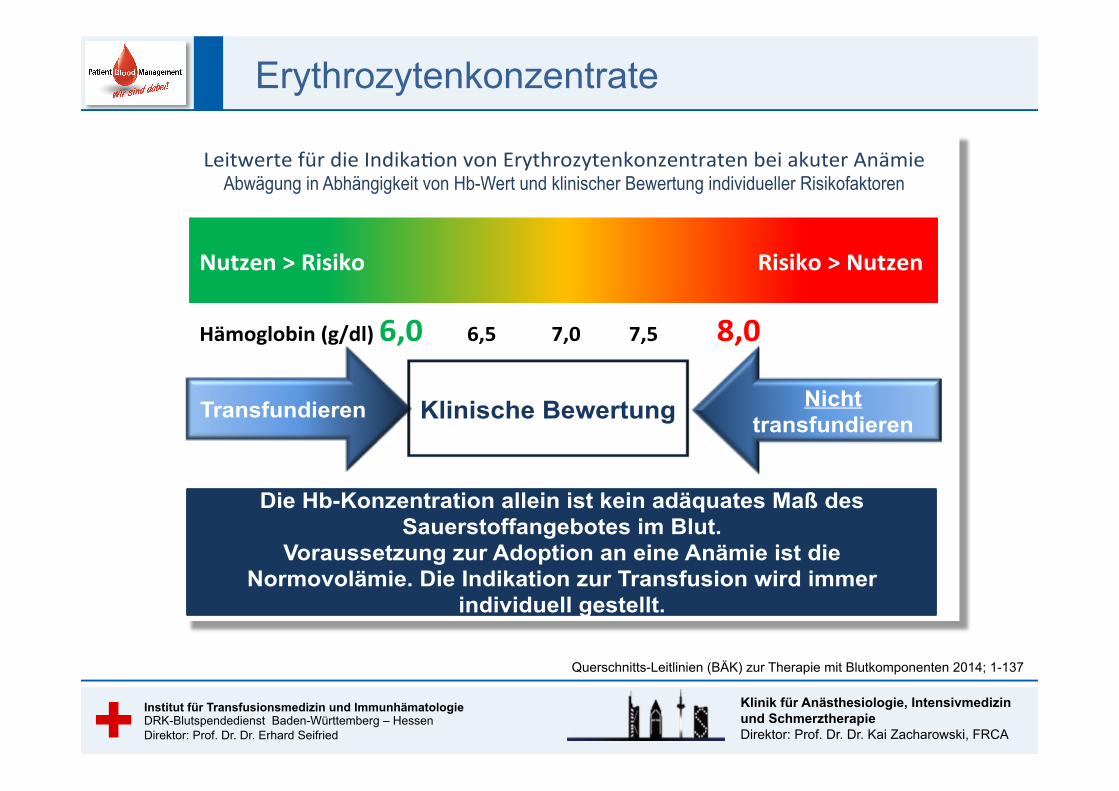
Querschnitts-Leitlinien (BÄK) zur Therapie mit Blutkomponenten 2014; 1-137
Erythrozytenkonzentrate
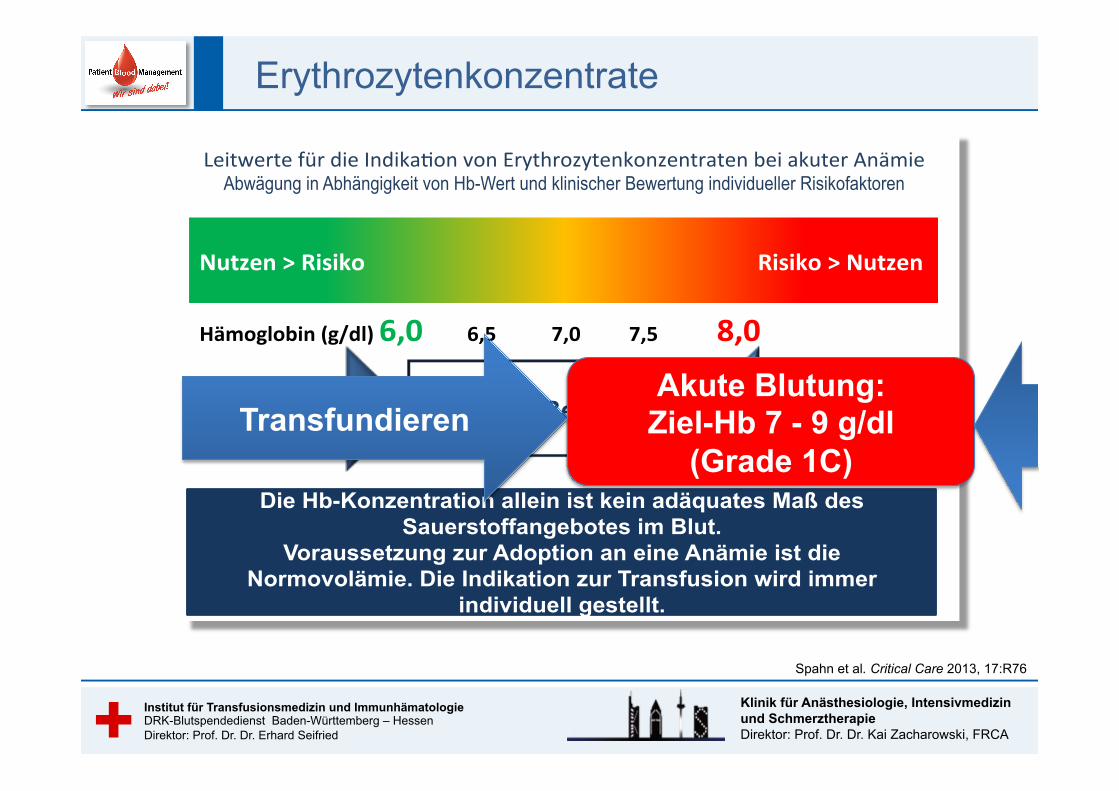
Leitwerte'für'die'Indika/on'von'Erythrozytenkonzentraten'bei'akuter'Anämie'Abwägung in Abhängigkeit von Hb-Wert und klinischer Bewertung individueller Risikofaktoren
Transfundieren Klinische Bewertung Nicht transfundieren
Die Hb-Konzentration allein ist kein adäquates Maß des Sauerstoffangebotes im Blut.
Voraussetzung zur Adoption an eine Anämie ist die Normovolämie. Die Indikation zur Transfusion wird immer
individuell gestellt.
Ergänzende Farbe grau: R = 100 G = 100 B = 100
Institut für Transfusionsmedizin und Immunhämatologie DRK-Blutspendedienst Baden-Württemberg – Hessen Direktor: Prof. Dr. Dr. Erhard Seifried
Klinik für Anästhesiologie, Intensivmedizin und Schmerztherapie Direktor: Prof. Dr. Dr. Kai Zacharowski, FRCA
Spahn et al. Critical Care 2013, 17:R76
Erythrozytenkonzentrate
Leitwerte'für'die'Indika/on'von'Erythrozytenkonzentraten'bei'akuter'Anämie'Abwägung in Abhängigkeit von Hb-Wert und klinischer Bewertung individueller Risikofaktoren
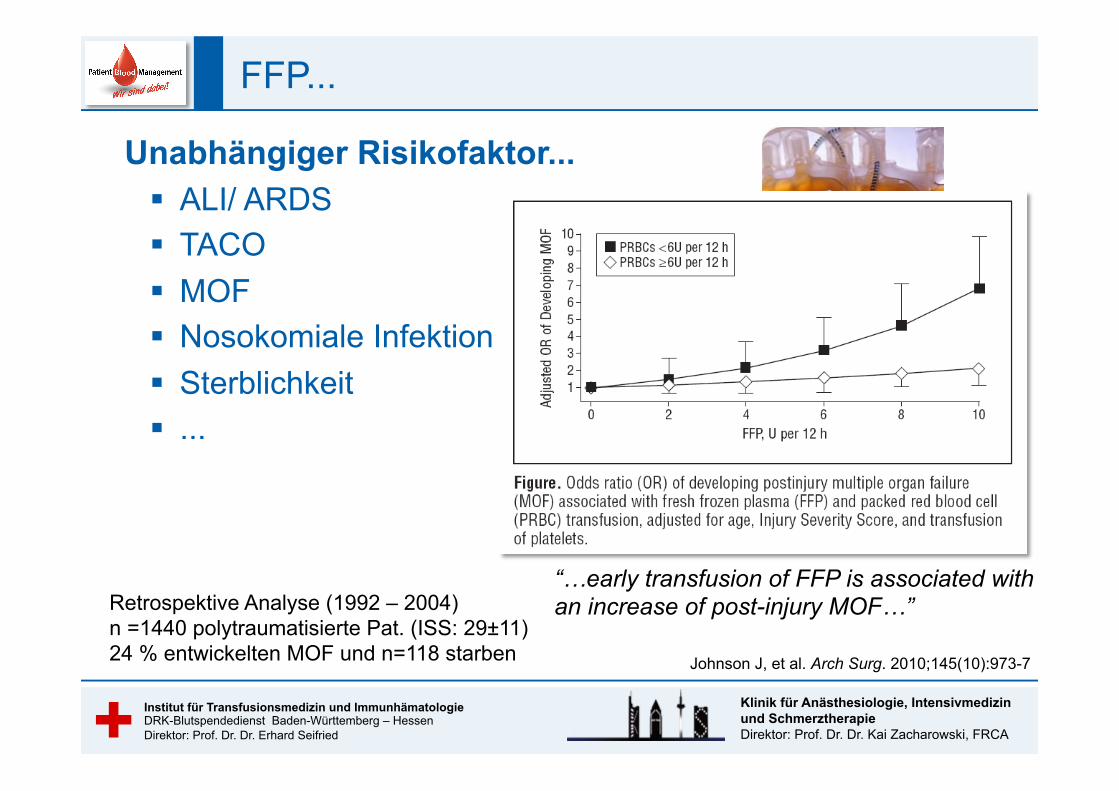
Retrospektive Analyse (1992 – 2004) n =1440 polytraumatisierte Pat. (ISS: 29±11) 24 % entwickelten MOF und n=118 starben
“…early transfusion of FFP is associated with an increase of post-injury MOF…”
Ergänzende Farbe grau: R = 100 G = 100 B = 100
Institut für Transfusionsmedizin und Immunhämatologie DRK-Blutspendedienst Baden-Württemberg – Hessen Direktor: Prof. Dr. Dr. Erhard Seifried
Klinik für Anästhesiologie, Intensivmedizin und Schmerztherapie Direktor: Prof. Dr. Dr. Kai Zacharowski, FRCA
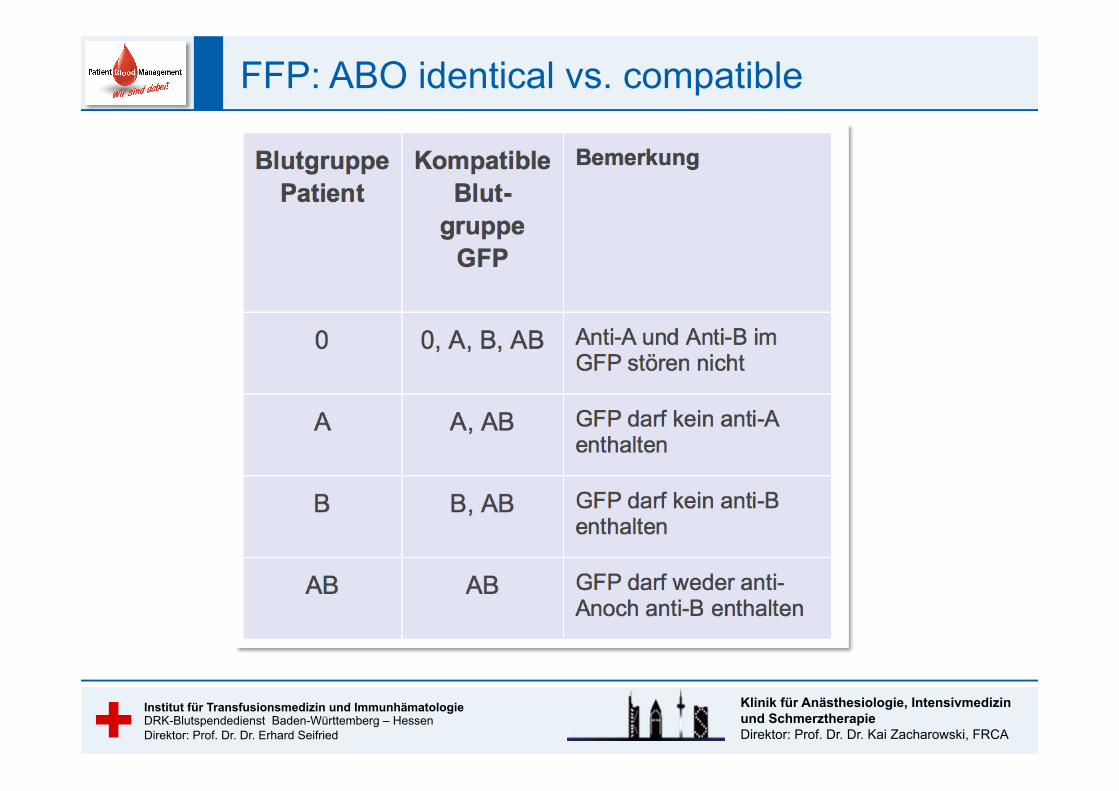
FFP: ABO identical vs. compatible
Ergänzende Farbe grau: R = 100 G = 100 B = 100
Institut für Transfusionsmedizin und Immunhämatologie DRK-Blutspendedienst Baden-Württemberg – Hessen Direktor: Prof. Dr. Dr. Erhard Seifried
Klinik für Anästhesiologie, Intensivmedizin und Schmerztherapie Direktor: Prof. Dr. Dr. Kai Zacharowski, FRCA
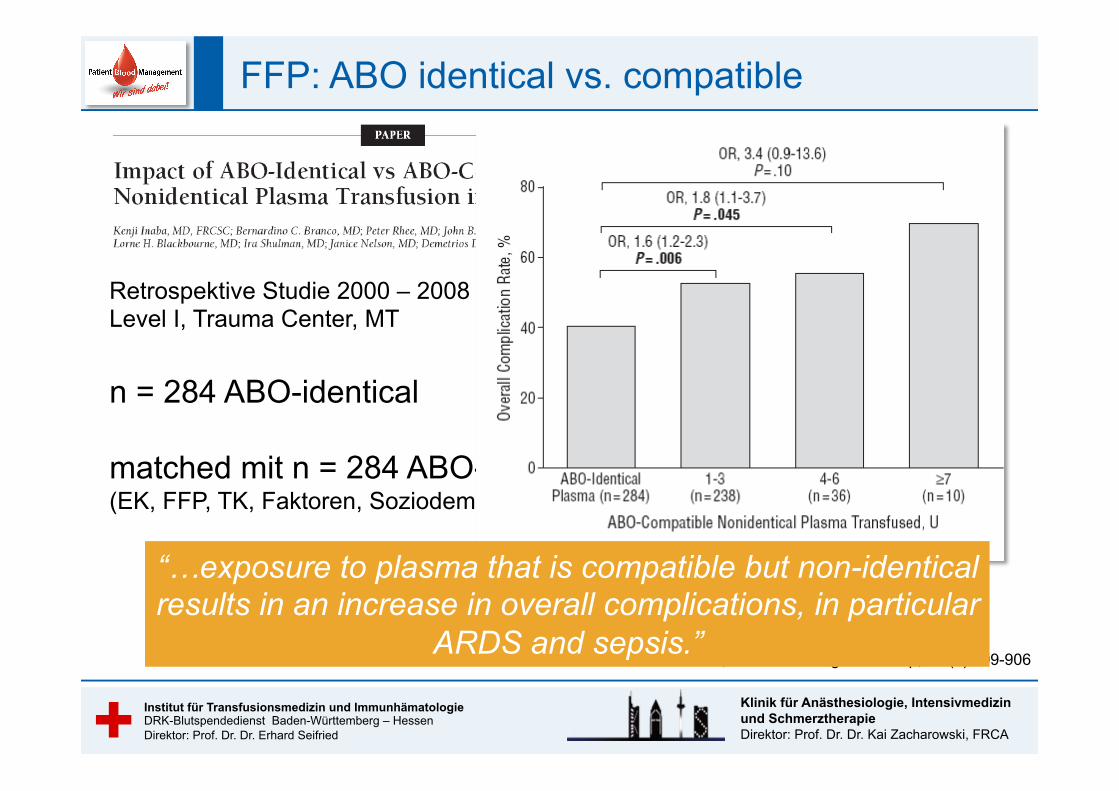
Inaba K, et al. Arch Surg. 2010 Sep;145(9):899-906
Retrospektive Studie 2000 – 2008 Level I, Trauma Center, MT n = 284 ABO-identical matched mit n = 284 ABO-compatible (EK, FFP, TK, Faktoren, Soziodemographic, Blutverlust) “…exposure to plasma that is compatible but non-identical
results in an increase in overall complications, in particular ARDS and sepsis.”
FFP: ABO identical vs. compatible
Ergänzende Farbe grau: R = 100 G = 100 B = 100
Institut für Transfusionsmedizin und Immunhämatologie DRK-Blutspendedienst Baden-Württemberg – Hessen Direktor: Prof. Dr. Dr. Erhard Seifried
Klinik für Anästhesiologie, Intensivmedizin und Schmerztherapie Direktor: Prof. Dr. Dr. Kai Zacharowski, FRCA
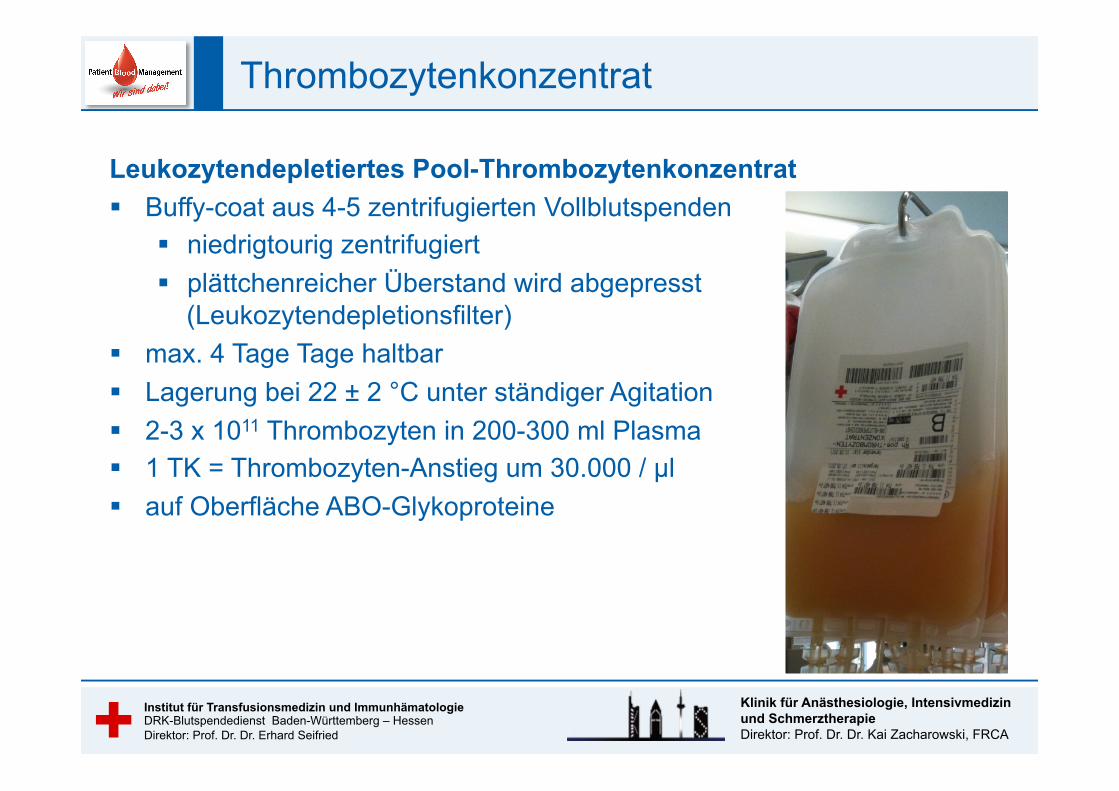
Thrombozytenkonzentrat
Leukozytendepletiertes Pool-Thrombozytenkonzentrat § Buffy-coat aus 4-5 zentrifugierten Vollblutspenden
§ niedrigtourig zentrifugiert § plättchenreicher Überstand wird abgepresst
(Leukozytendepletionsfilter) § max. 4 Tage Tage haltbar § Lagerung bei 22 ± 2 °C unter ständiger Agitation § 2-3 x 1011 Thrombozyten in 200-300 ml Plasma § 1 TK = Thrombozyten-Anstieg um 30.000 / µl § auf Oberfläche ABO-Glykoproteine
Ergänzende Farbe grau: R = 100 G = 100 B = 100
Institut für Transfusionsmedizin und Immunhämatologie DRK-Blutspendedienst Baden-Württemberg – Hessen Direktor: Prof. Dr. Dr. Erhard Seifried
Klinik für Anästhesiologie, Intensivmedizin und Schmerztherapie Direktor: Prof. Dr. Dr. Kai Zacharowski, FRCA
Thrombozytenkonzentrat
Ergänzende Farbe grau: R = 100 G = 100 B = 100
Institut für Transfusionsmedizin und Immunhämatologie DRK-Blutspendedienst Baden-Württemberg – Hessen Direktor: Prof. Dr. Dr. Erhard Seifried
Klinik für Anästhesiologie, Intensivmedizin und Schmerztherapie Direktor: Prof. Dr. Dr. Kai Zacharowski, FRCA
Thrombozytenkonzentrat
„Human-Thrombozytenkonzentrat“ § Gepoolt aus 4 Vollblutspenden § leukozytendepletiert § in CPD-Stabilisatorlösung § max. 4 Tage Tage haltbar § Lagerung bei 22 ± 2 °C § gleichmäßige Agitation („Schütteln“) § 2–4 x 1011 Thrombozyten/Unit § auf Oberfläche ABO-Glykoproteine
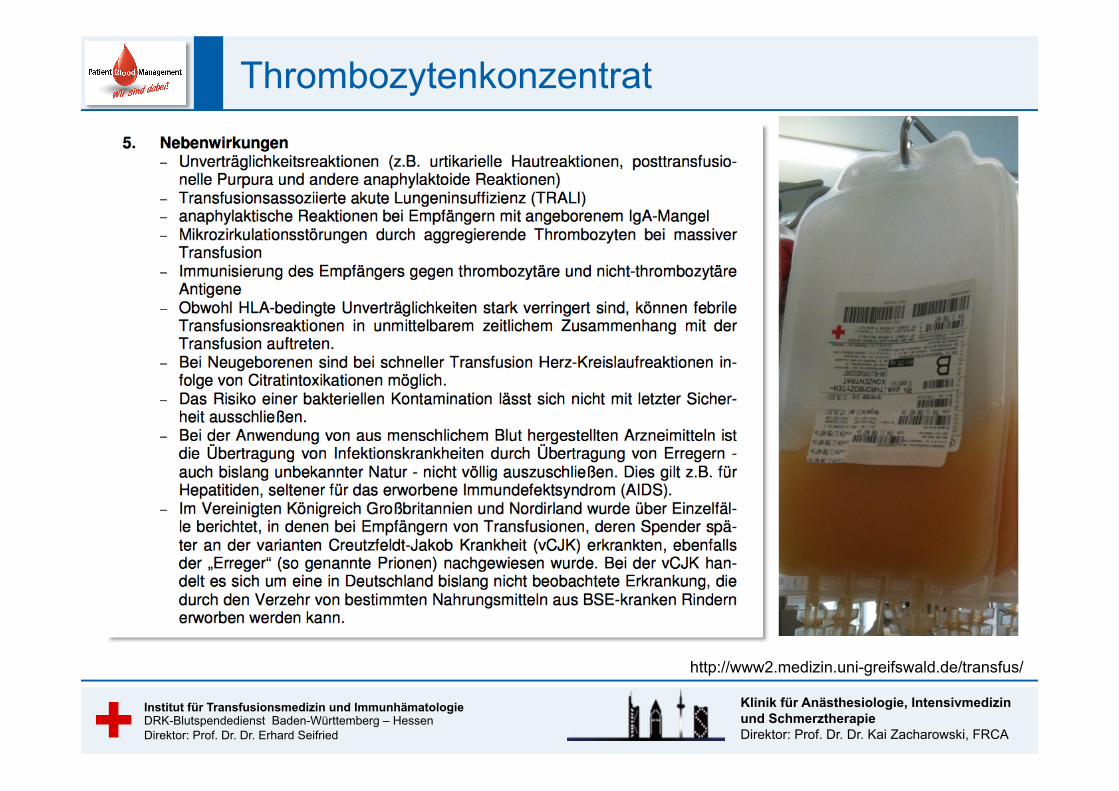
http://www2.medizin.uni-greifswald.de/transfus/
Ergänzende Farbe grau: R = 100 G = 100 B = 100
Institut für Transfusionsmedizin und Immunhämatologie DRK-Blutspendedienst Baden-Württemberg – Hessen Direktor: Prof. Dr. Dr. Erhard Seifried
Klinik für Anästhesiologie, Intensivmedizin und Schmerztherapie Direktor: Prof. Dr. Dr. Kai Zacharowski, FRCA
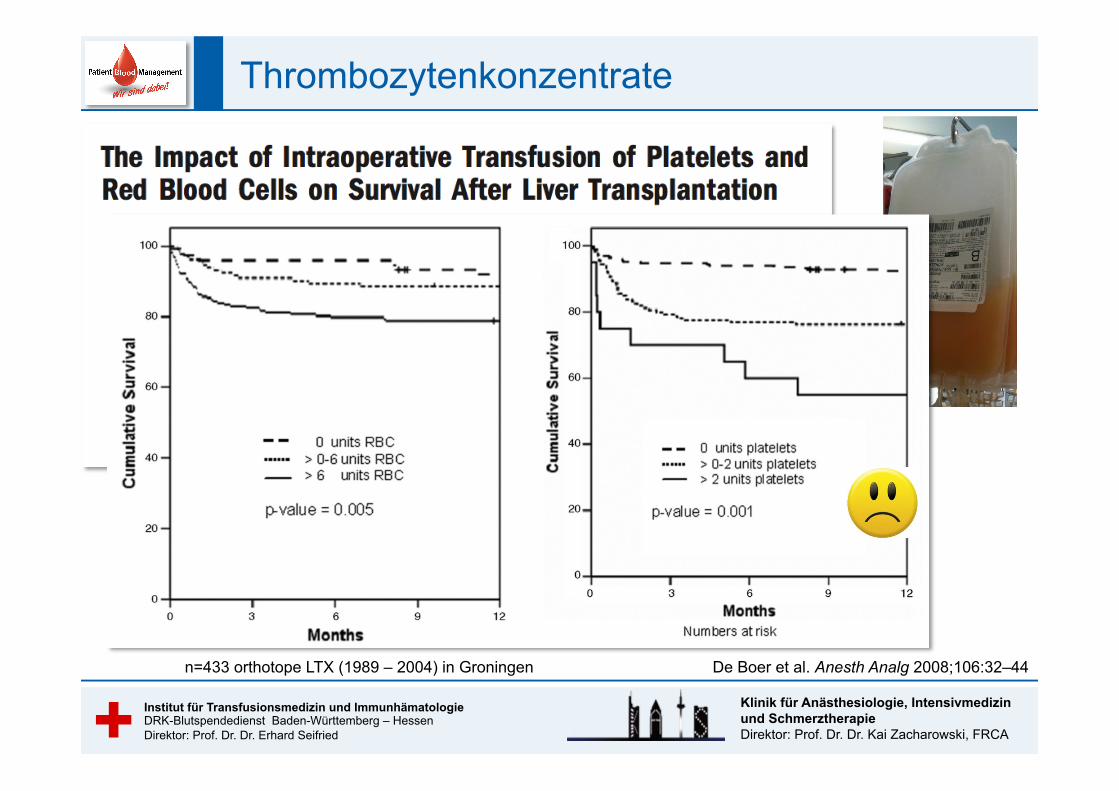
Thrombozytenkonzentrate
n=433 orthotope LTX (1989 – 2004) in Groningen
De Boer et al. Anesth Analg 2008;106:32–44
Ergänzende Farbe grau: R = 100 G = 100 B = 100
Institut für Transfusionsmedizin und Immunhämatologie DRK-Blutspendedienst Baden-Württemberg – Hessen Direktor: Prof. Dr. Dr. Erhard Seifried
Klinik für Anästhesiologie, Intensivmedizin und Schmerztherapie Direktor: Prof. Dr. Dr. Kai Zacharowski, FRCA
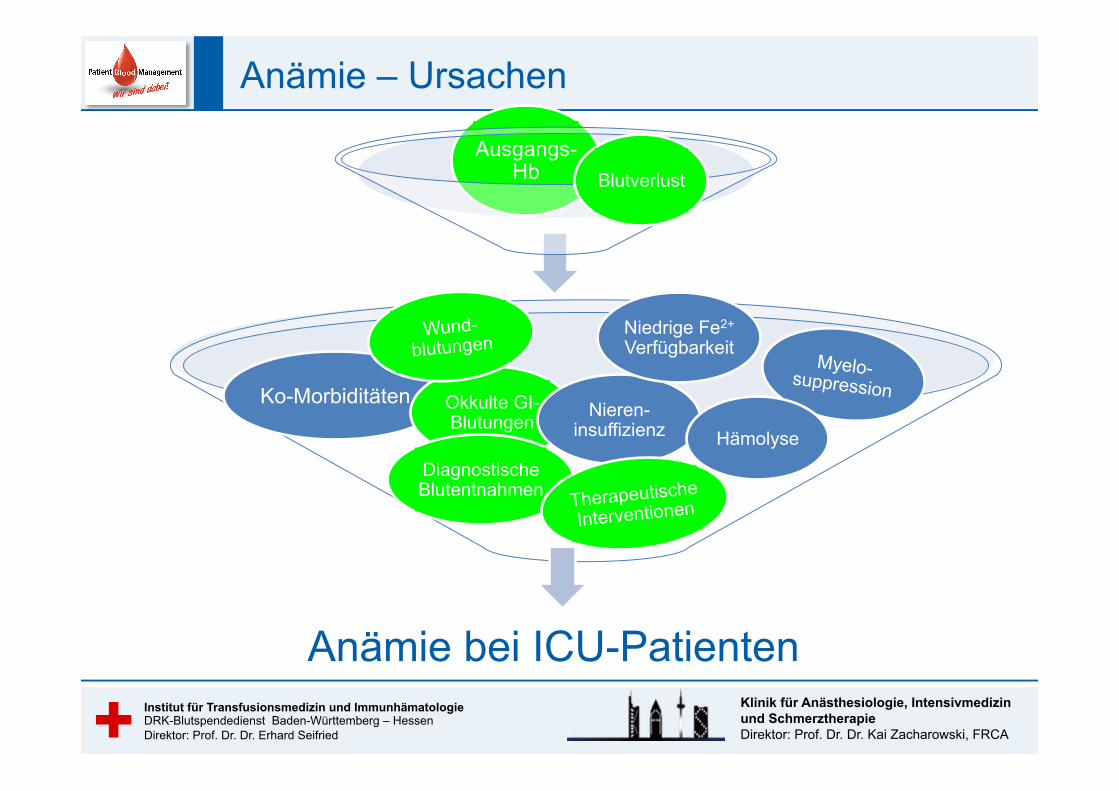
Anämie – Ursachen
Ausgangs-Hb Blutverlust
Ko-Morbiditäten Okkulte GI-Blutungen
Wund-blutungen
Nieren-insuffizienz
Niedrige Fe2+ Verfügbarkeit
Myelo-suppression
Diagnostische Blutentnahmen
Hämolyse
Therapeutische
Interventionen
Anämie bei ICU-Patienten
Ergänzende Farbe grau: R = 100 G = 100 B = 100
Institut für Transfusionsmedizin und Immunhämatologie DRK-Blutspendedienst Baden-Württemberg – Hessen Direktor: Prof. Dr. Dr. Erhard Seifried
Klinik für Anästhesiologie, Intensivmedizin und Schmerztherapie Direktor: Prof. Dr. Dr. Kai Zacharowski, FRCA
Institut für Transfusionsmedizin und Immunhämatologie DRK-Blutspendedienst Baden-Württemberg – Hessen Direktor: Prof. Dr. Dr. Erhard Seifried
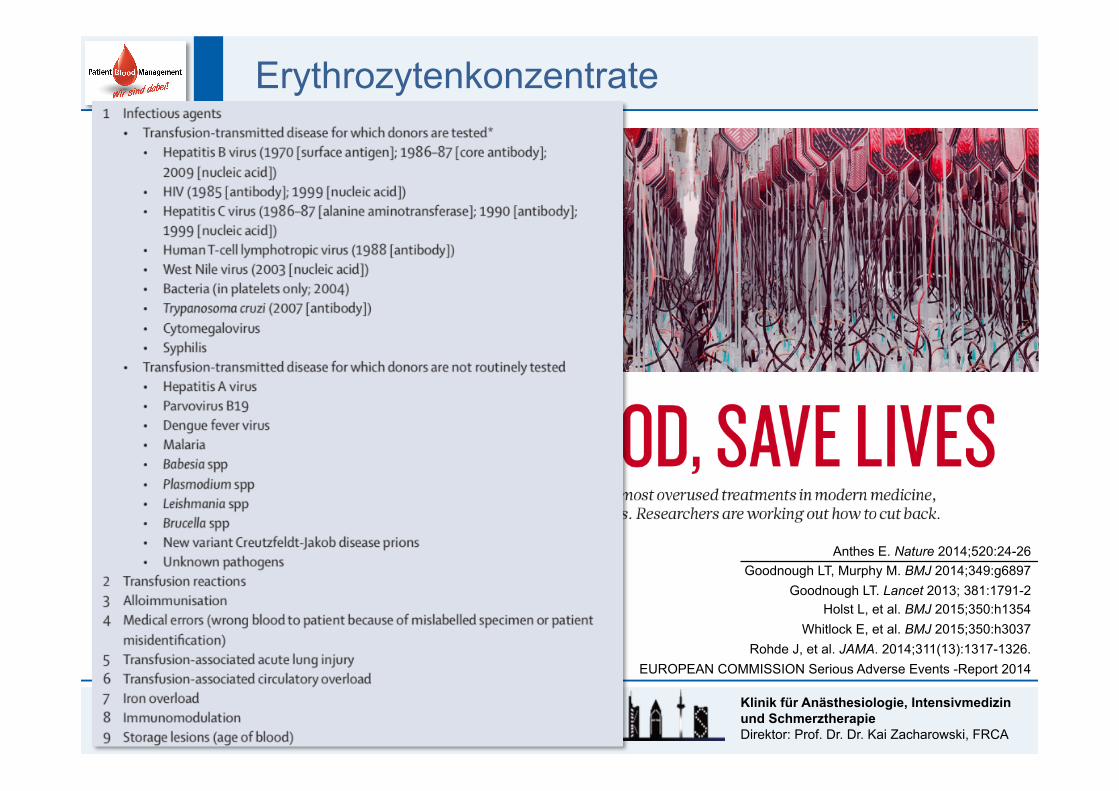
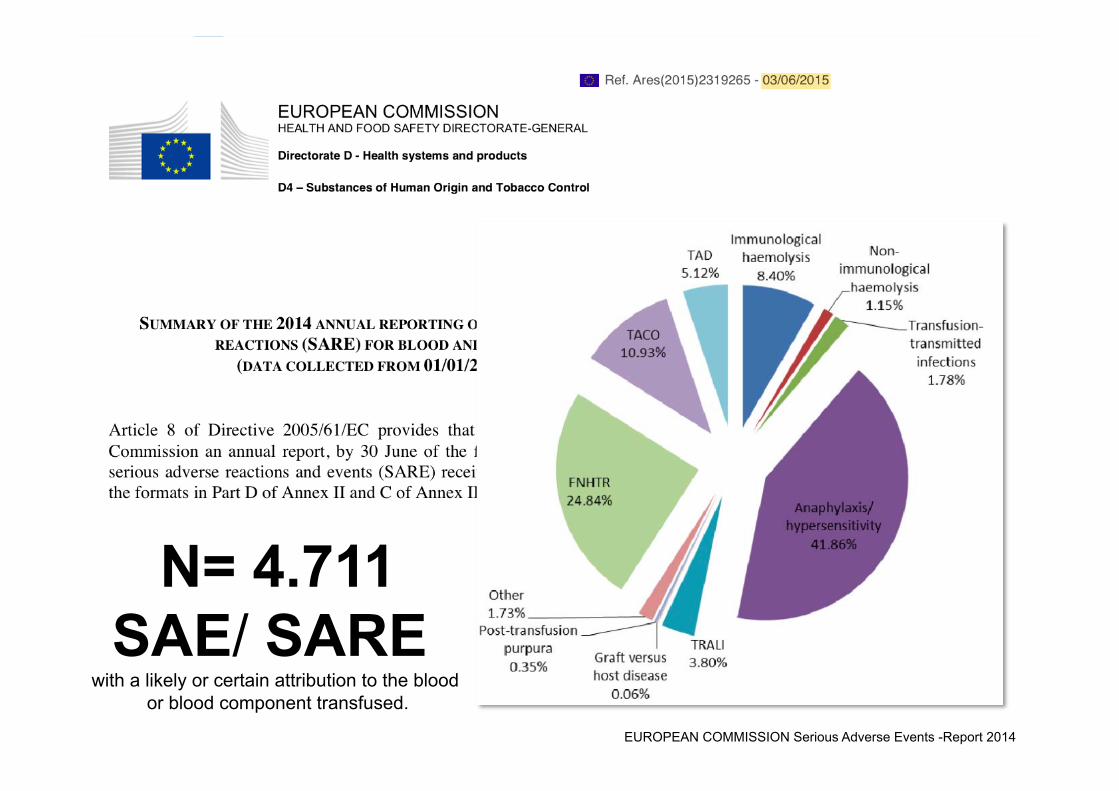
Klinik für Anästhesiologie, Intensivmedizin und Schmerztherapie Direktor: Prof. Dr. Dr. Kai Zacharowski, FRCA EUROPEAN COMMISSION Serious Adverse Events -Report 2014
N= 4.711 SAE/ SARE
with a likely or certain attribution to the blood or blood component transfused.